SSSS
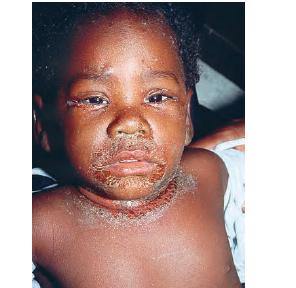
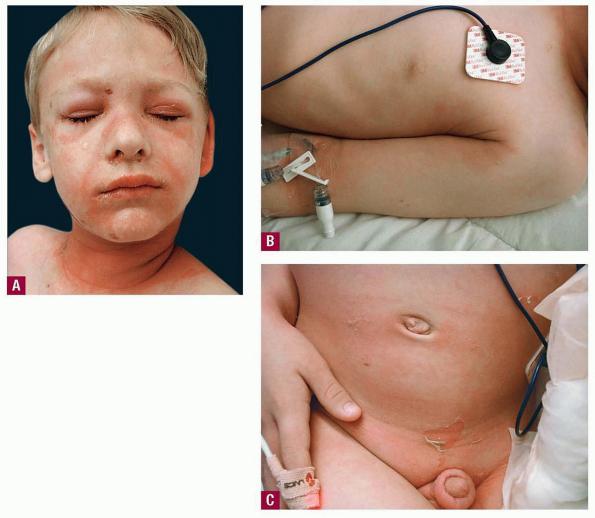
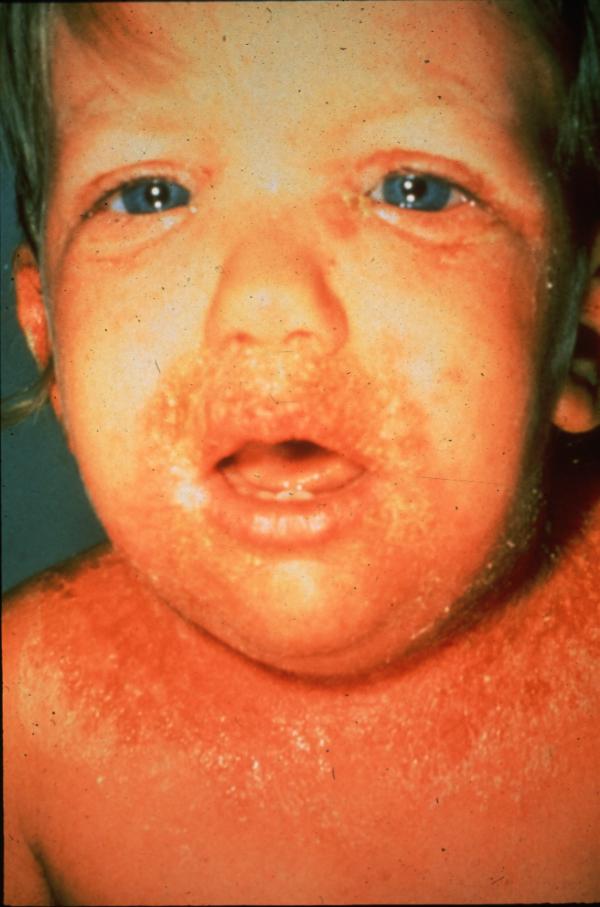
The clinical features of SSSS were first described in 1878 by the German physician Gotfried Ritter von Rittershain, who reported almost 300 cases of “dermatitis exfoliativa neonatorum” among young children. Outbreaks of SSSS tend to occur in clusters as a consequence of cross-infection. Typically neonatal or maternity hospital staff colonized or infected with ET-producing staphylococci are the source of these outbreaks. Although more commonly seen in infants/children, SSSS can also be seen in adults. The risk factors for adults include a compromised immune response allowing for growth of the S. aureus and possibly impaired amounts of toxin-neutralizing antibodies or renal insufficiency, which decreases the clearance of the toxin. Affected individuals initially have a faint, orange-red macular exanthem or uniform erythema sparing mucosal surfaces in association with a purulent conjunctivitis, otitis media, nasopharyngeal infection, or, occasionally, pyogenic skin infection such as bullous impetigo or that which arises from an umbilical stump or boil (carbuncle). These are the staphylococcal foci from which the toxin is released. Periorificial and flexural accentuation of the exanthema is often noted.
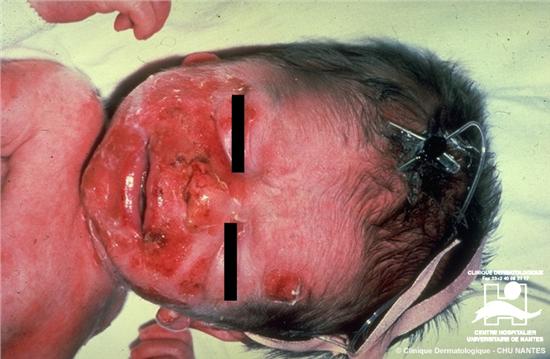
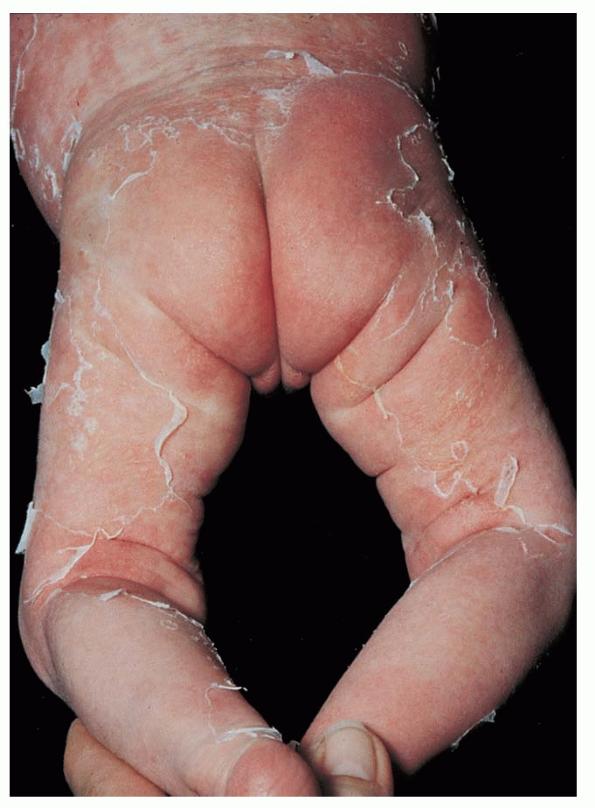
Although the early rash is not distinctive in appearance, the concomitant cutaneous tenderness is usually present at this early stage. Tenderness can be often so severe that infants will refuse to lie down or allow anyone to hold them. Within 1 to 2 days the rash progresses from an exanthematous scarlatiniform to a blistering eruption . Very superficial tissue paper-like wrinkling of the epidermis, which is characteristic, progresses to large flaccid bullae in flexural and periorificial surfaces. A positive Nikolsky sign can be elicited by stroking the skin, which results in a superficial blister . Large sheets of the epidermal surface are typically shed, revealing a moist underlying erythematous base. At this stage, the disease looks very worrisome, resembling a generalized scalding burn. Although fevers are often present and outwardly the signs of SSSS may look serious, the infants and children do not usually appear toxic unless they have developed complications such as septicemia or pneumonia. The cutaneous process usually resolves spontaneously or faster with antibiotics and superficial desquamation, with healing complete within 5 to 7 days . Cultures obtained from an intact blister are usually sterile consistent with the pathogenesis of a hematogenously disseminated toxin originating from a distant focus of infection.
Although most cases of SSSS occur in infants and children, the syndrome can also rarely be seen in adults, particularly when there is renal failure . Histopathology shows acantholysis in the granular layer and sub-corneal cleft formation in early lesions and an intact viable epidermis with shedding of the stratum corneum in the desquamative stage.
INTERMEDIATE (ABORTIVE) FORMS
In addition to localized bullous impetigo and generalized SSSS, intermediate forms of staphylococcal-mediated eruptions, in which blistering can be apparent, can be encountered. One scenario is localized bullous impetigo that evolves to produce regionally limited bullae and denuded areas that may or may not actually harbor S. aureus. A possibly abortive form of SSSS has been described. It is known as the scarlatiniform variant and has features of the early erythrodermic and final desquamative stages yet very little blister formation is present (see Staphylococcal Scarlet Fever). Again, because S. aureus bacterial strains can produce both exfoliative and other superantigenic toxins, and ETs could have superantigenic activity, it is not surprising that overlap syndromes with features of toxic shock and scalded skin can infrequently be observed.
Diagnosis and Differential Diagnosis
All forms of SSSS are characterized by intraepidermal cleavage with splitting beneath and within the stratum granulosum. The cleavage space may contain either partially or totally unattached acantholytic cells. However, the remainder of the epidermis is usually unremarkable, and the dermis contains few inflammatory cells . In localized bullous impetigo, more inflammatory cells, including neutrophils, can be often visualized .
The principal diagnostic problem is distinguishing generalized SSSS from toxic epidermal necrolysis (TEN) . It should be noted that the cases that represented Lyell's first description of TEN actually included some that were probably SSSS. The age distribution between SSSS (neonates, children) and TEN tends to be different, yet much overlap occurs. In contrast to TEN, SSSS never has mucosal erosions. Using a Tzanck smear that will show acantholytic cells in SSSS but not in TEN and the use of frozen sections that can rapidly differentiate the superficial subgranular acantholysis in SSSS versus the characteristic full-thickness epidermal necrosis and dermal-epidermal separation seen in TEN aid in the differential diagnosis.
Treatment and Prognosis
Therapy for bullous impetigo may include topical mupirocin ointment therapy alone and/or oral antibiotics. Prognosis for recovery is excellent. Therapy for SSSS should be directed toward eradication of S. aureus, which generally requires hospitalization and intravenous anti-staphylococcal antibiotics. For uncomplicated cases, oral antibiotics can usually be substituted after several days. The use of suitable antibiotics combined with supportive skin care and management of potential fluid and electrolyte abnormalities due to the widespread disruption of barrier function will usually be sufficient to ensure rapid recovery. Neonates benefit from incubators to maintain body temperature and humidity. The use of non-adherent dressings, including petrolatum-impregnated gauze, to the widespread areas of superficial blistering are helpful. Antibiotic mupirocin ointment applied several times per day to clearly impetiginized areas, including the original source, is often a helpful adjunct to systemic antibiotic therapy.
Major complications of SSSS are serious fluid and electrolyte disturbances. The mortality in uncomplicated pediatric SSSS is very low (2 percent) and is not usually associated with sepsis. Adult mortality is higher (approximately 10 percent) due to concomitant morbidity factors and increased likelihood of sepsis.