|
Pretibial myxedema = الوذمة المخاطية أمام الظنبوب |
 |
 |
 |
|
Pretibial Myxedema
Usually, the lesions are limited to the anterior aspects of the legs, but they may extend to the dorsa of the feet. They consist of raised, nodular, yellow, waxy plaques with prominent follicular openings that give a peau d'orange appearance . Similar lesions rarely occur on the radial aspect of the forearms .
|
|
Pretibial myxedema usually occurs in association with thyrotoxicosis and not infrequently becomes more pronounced after treatment of the thyrotoxicosis. It nearly always occurs in association with exophthalmos, and 15% to 20% also have acropachy . Complete remission occurs in about 25% of cases . Rarely, pretibial myxedema, with or without exophthalmos, occurs in nonthyrotoxic thyroid disease such as chronic lymphocytic thyroiditis; the patient is then either euthyroid or hypothyroid .
|
|
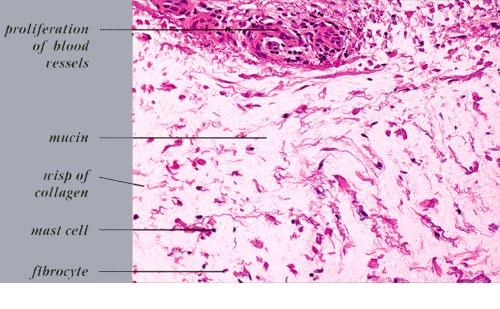
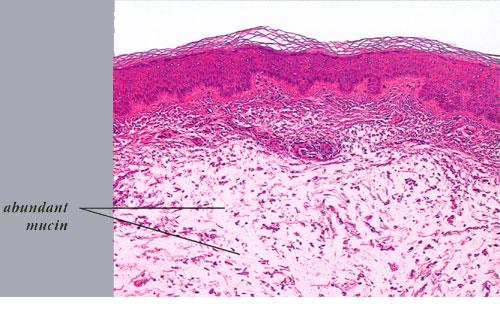
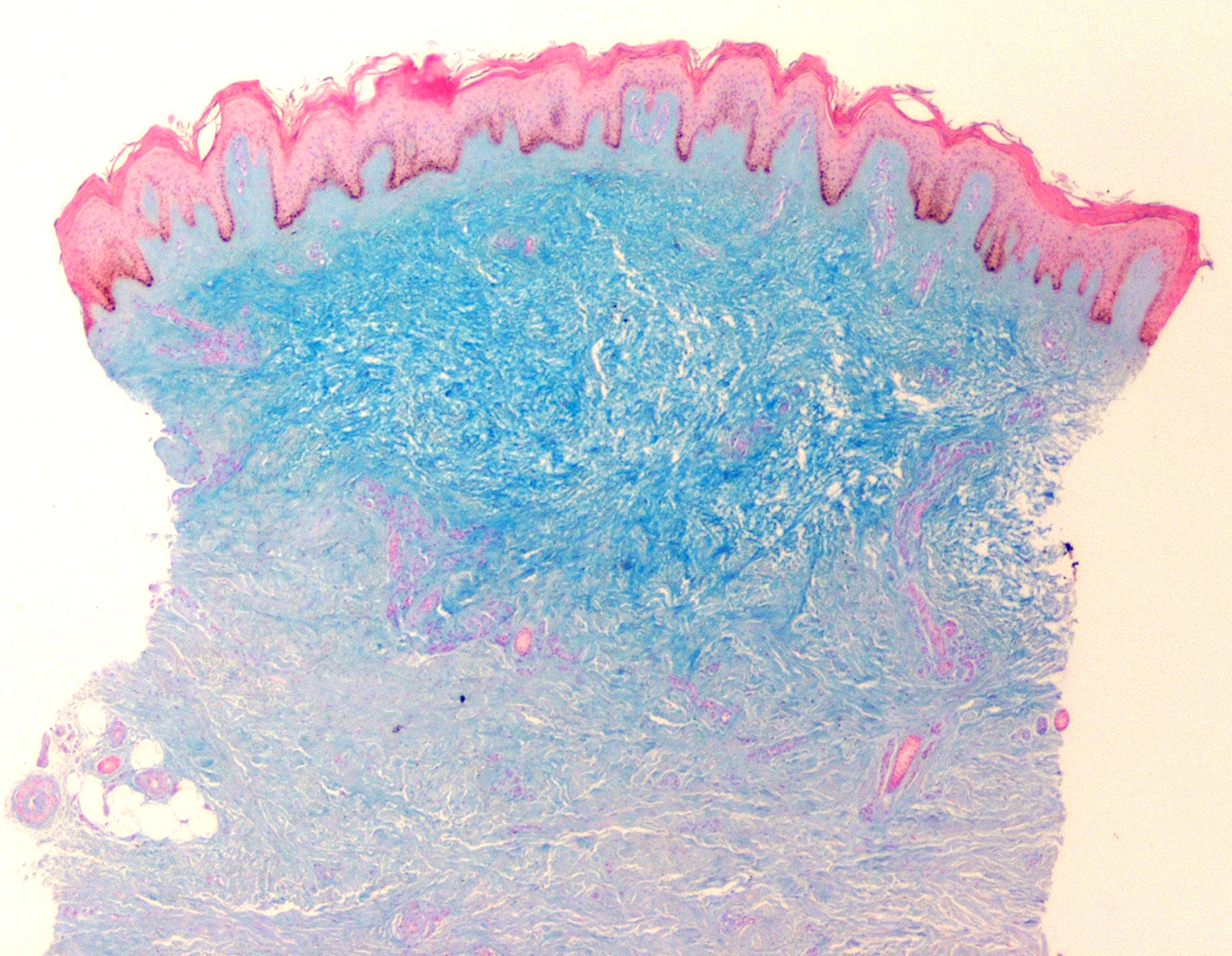
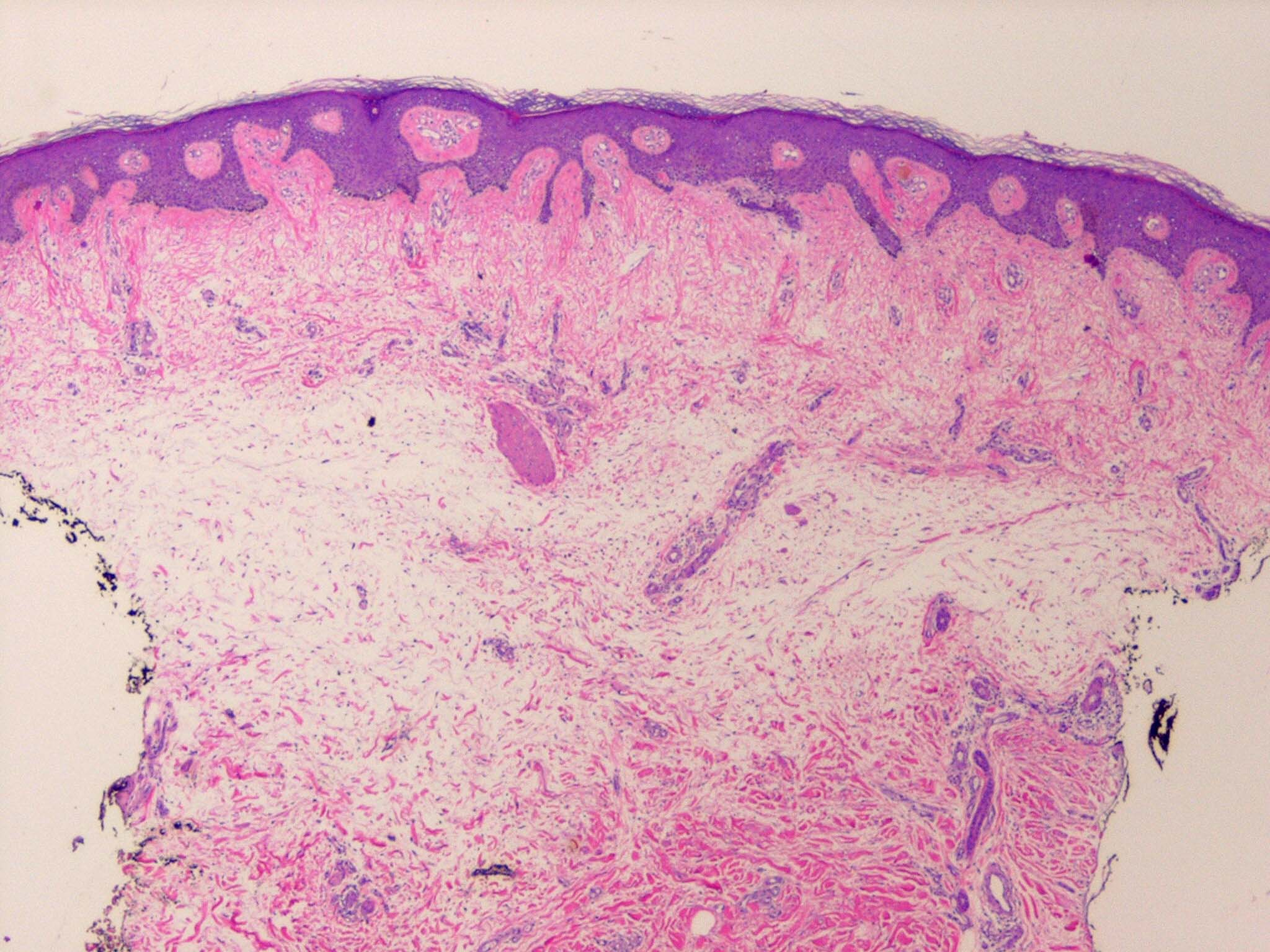
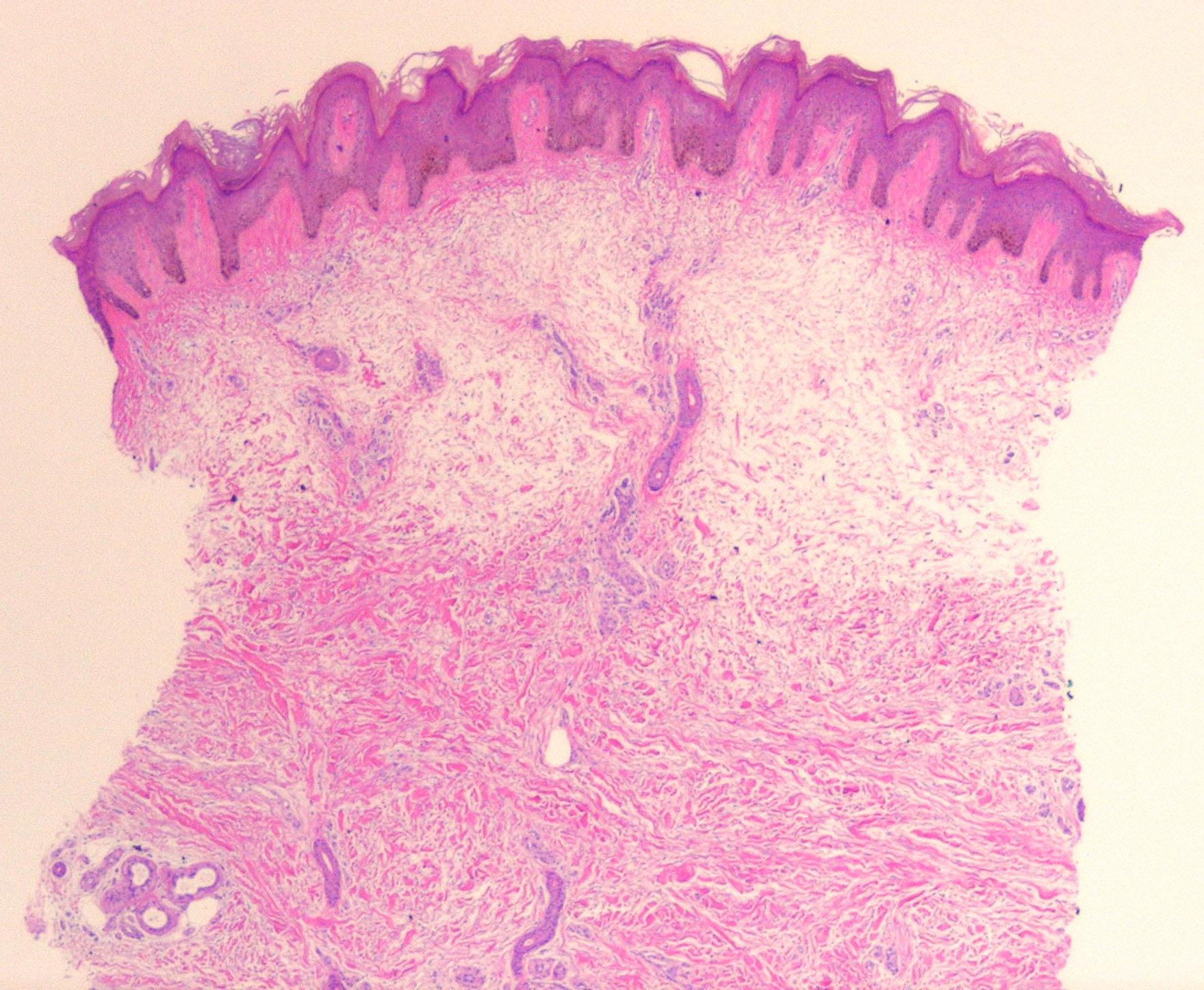
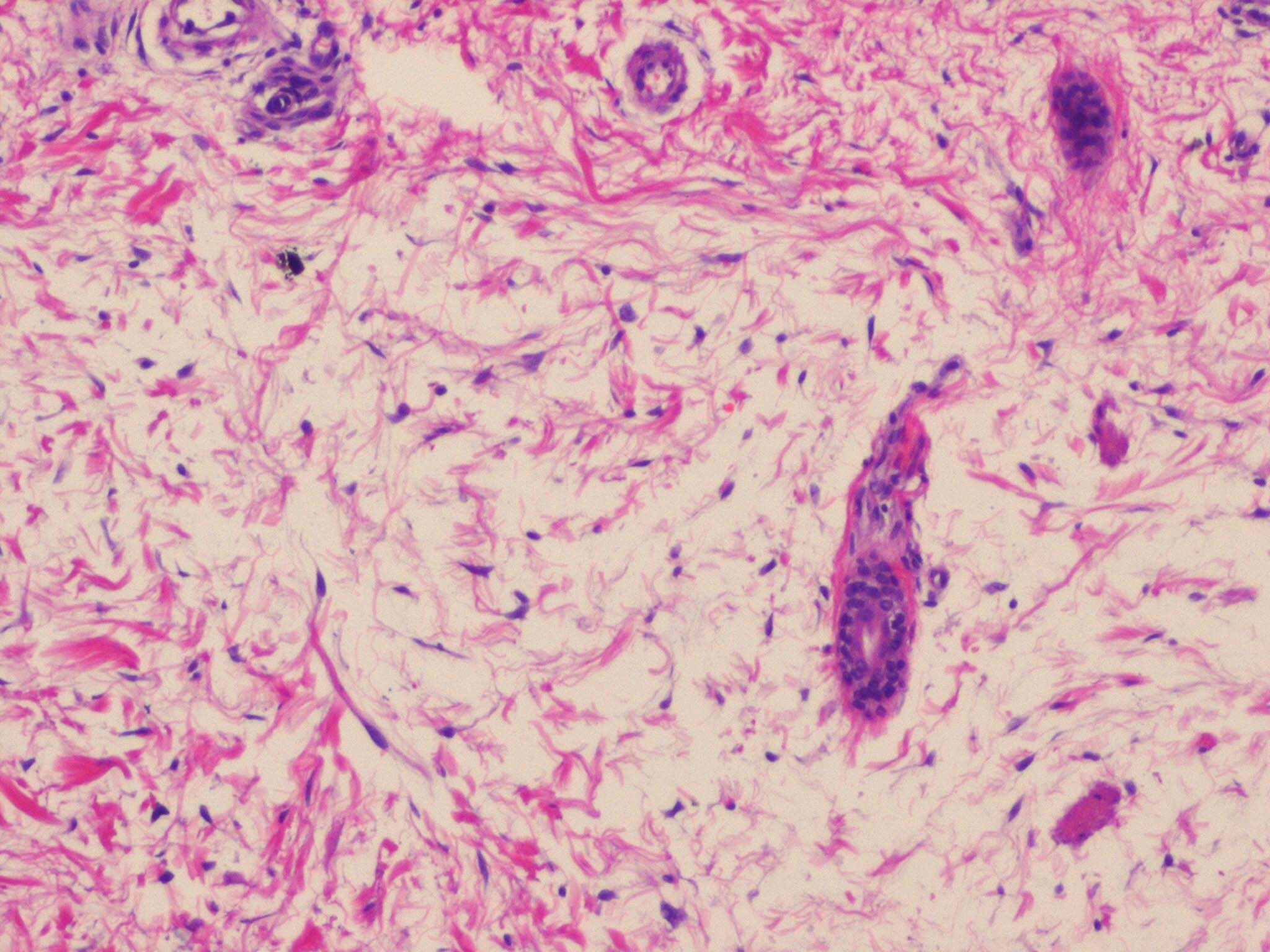
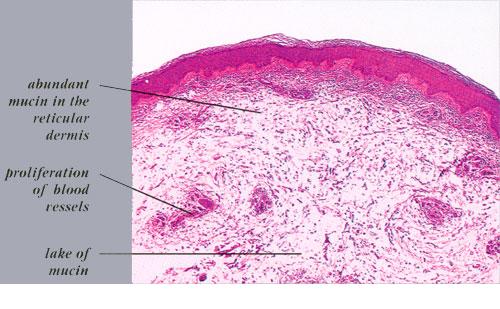
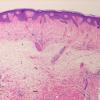
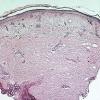
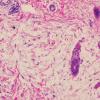
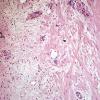
Histopathology.
The epidermis and papillary dermis are usually normal. Mucin in large amounts is present in the dermis,
|
|
particularly in the upper half . As a result, the dermis is greatly thickened. The mucin occurs not only as individual threads and granules but also as extensive deposits resulting in the splitting up of collagen bundles into fibers and wide separation of the fibers. As a result of shrinkage of the mucin during the process of fixation and dehydration, there are empty spaces within the mucin deposits. The number of fibroblasts is not increased as a rule, but in areas where there is much mucin, some fibroblasts have a stellate shape and are then referred to as mucoblasts . A perivascular infiltrate of lymphocytes may be seen in some cases, and mast cells are moderately increased in number .
|
|
Pathogenesis. On electron microscopic examination, the collagen bundles and fibers are separated by wide,
|
|
electron-lucent, empty spaces. The fibroblasts that produce the mucin are stellate shaped with long, thin cytoplasmic processes and exhibit dilated cisternae of the rough endoplasmic reticulum. An amorphous, moderately electron-dense material coats the surface of the fibroblasts. This material is also present in small, irregular clumps within the otherwise empty-appearing spaces . At high magnification, the amorphous material appears as a complex of microfibrils and granules, forming a network .
|
|
Of interest is the almost invariable presence of long-acting thyroid stimulator (LATS) in the serum of patients with pretibial myxedema. There is, however, a rather poor correlation between the severity of the skin lesions and the level of serum LATS; furthermore, LATS is detected in 40% to 60% of patients with an active exophthalmic goiter but without pretibial myxedema. Thus, LATS cannot be regarded as the cause of pretibial myxedema . It is likely that the IgG LATS represents an autoantibody that is produced by lymphocytes in thyroid disease, especially in thyrotoxicosis, and is a reflection rather than a cause of the underlying disease .
The restriction of the myxedema largely to the pretibial area may be explained by the finding that fibroblasts from the pretibial area synthesize two to three times more hyaluronic acid than do fibroblasts from other areas when incubated with serum from patients with pretibial myxedema . The receptor for thyroid-stimulating hormone (TSH-R) is a candidate as the common tissue antigen in Grave's disease, exophthalmos, and pretibial myxedema. TSH-R immunoreactivity has been detected on fibroblasts in the dermis of control patients without thyroid disease .
|
|
Differential Diagnosis. Pretibial myxedema must be differentiated from pretibial mucinosis associated with venous stasis. In pretibial mucinosis, the excess mucin is localized to the thickened papillary dermis and is accompanied by angioplasia and siderophages .
|
|