|
Palmoplantar keratoderma = التقرن الجلدي الراحي الاخمصي |
|
|
Keratosis Palmaris ET Plantaris
|
|
Three major autosomal dominant forms and two autosomal recessive forms of keratosis palmaris et plantaris exist. Evidence is accruing that indicates abnormalities in intracellular structural proteins {e.g., loricrin, keratins}, desmosomal proteins, gap junction components {e.g., connexins}, and enzymes {e.g., cathepsins} lead to the varying palmoplantar keratodermas. Gene defects causing many types of hereditary palmoplantar keratodermas have been discovered {63}. The three dominantly inherited forms include the following:
|
|
1. Keratosis palmaris et plantaris of Unna- Thost,
showing either diffuse or localized, occasionally linear hyperkeratosis of the palms and soles {Fig. 6-6}. A division into two types-a circumscribed type with limitation to the palms and soles and an extending type with gradual progression to the dorsa of the hands and feet, the ankles and wrists, and the elbows and knees-is not tenable, because both types may occur in the same family .
|
|
2. Epidermolytic keratosis palmaris et plantaris, although clinically indistinguishable from the Unna- Thost type, histologically shows epidermolytic hyperkeratosis. This form appears to be quite common {65}. This variant has been associated with mutations in keratin type 9 localized within the keratin gene cluster on chromosome 17q 12-q21 and keratin type 1 on chromosome 12q13 .
|
|
3. Keratosis palmoplantaris punctata {or papulosa} has multiple keratotic plugs.
|
|
The two recessively inherited forms include the following:
|
|
1. Keratosis palmaris et plantaris of the Meleda type, showing diffuse involvement of the palms and soles and a marked tendency toward progression to the dorsa of the hands and feet, the ankles and wrists, and the elbows and knees {67}.
|
|
2. The Papillon-Lefiwre syndrome shows the clinical characteristics of the Meleda type in association with periodontosis resulting in the loss first of the deciduous teeth and later of the permanent teeth {68}. Abnormalities in cathepsin C localized to chromosome 11q14.1 has been found as well as keratins 6b,9,16,17 on 12q13 and 17q12-q21 and connexin 30 on 13q12 .
|
|
In addition, keratosis palmaris et plantaris occurs in three syndromes: {a} pachyonychia congenita, {b} hidrotic ectodermal dysplasia, and {c} the Richner-Hanhart syndrome associated with tyrosinemia {tyrosine tyrosinase on
|
|
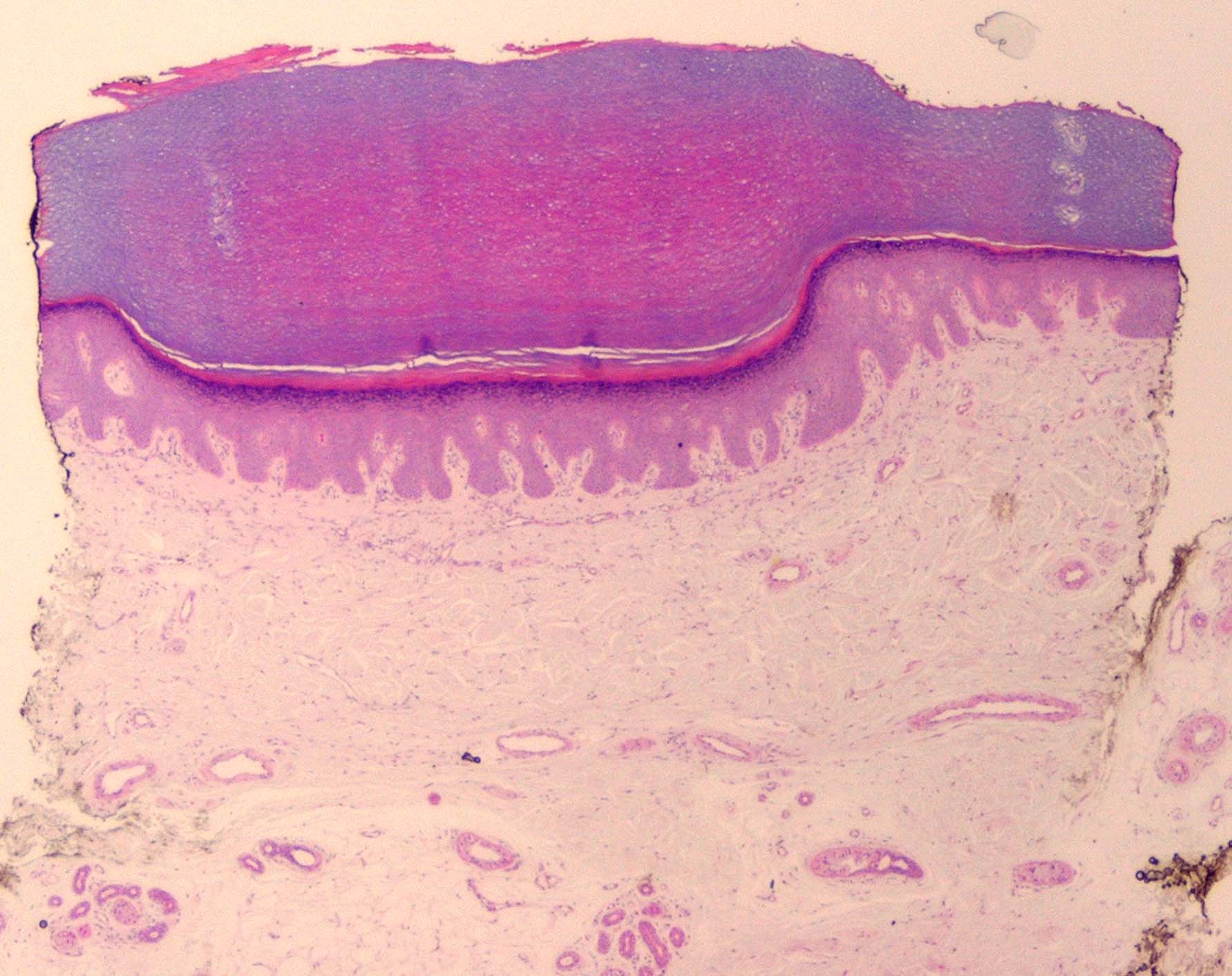
Histopathology.
In keratosis palmaris et plantaris of the Unna-Thost type and the Meleda type, as well as in the Papillon-Lefevre syndrome, the histologic picture is nonspecific, consisting of considerable hyperkeratosis, hypergranulosis, acanthosis, and a sparse inflammatory infiltrate of lymphocytes in the upper dermis .
|
|
In epidermolytic keratosis palmaris et plantaris, the histologic picture is identical with that seen in epidermolytic hyperkeratosis. Many cells in the middle and upper stratum malpighii appear vacuolated, and scattered cavities are present as a result of ruptured cell walls. Keratohyaline granules are numerous and large .
|
|
In keratosis palmoplantaris punctata, there is massive hyperkeratosis over a sharply limited area, with depression of the underlying malpighian layer below the general level of the epidermis. There is an increase in the thickness of the granular layer. The dermis is free of inflammation . In two cases reported as punctate keratoderma, a cornoid lamella was seen in the center of the hyperkeratotic plug; these cases represent punctate porokeratosis with the lesions limited to the palms and soles, rather than keratosis palmoplantaris punctata .
|
|

