

Lichen Nitidus
Lichen nitidus (Latin nitidus, “shiny” or “glistening”) is an uncommon, usually asymptomatic cutaneous eruption first described by Felix Pinkus in 1901 and further characterized by him in 1907. The dermatosis consists of small, glistening, flesh-colored to pink or reddish-brown papules that may be limited to the penis, genitalia, abdomen, and extremities or, less frequently, may occur as a generalized condition. The histopathologic findings are characteristic. Although the condition is often chronic, the prognosis is good, and no clearly associated systemic illnesses have been documented.
EPIDEMIOLOGY
Because the disease is uncommon, accurate epidemiologic characteristics of lichen nitidus have not yet been defined. Lichen nitidus is a dermatosis that occurs infrequently and has been reported to affect blacks more than Caucasians, although no strong predisposition for any race is clearly evident. Perhaps the relative prominence of pale lesions on dark skin accounts for the reported increased incidence in blacks. A predilection for children, young adults, and males has also been reported, but, again, these data are not well established. The incidence is estimated to be approximately 3.4 cases/10,000 population, based on a 25-year survey of skin diseases in African Americans. Compared to the more common lichen planus, the crude ratio of lichen nitidus to lichen planus is 1.7:100, based on pathologic diagnosis of cases evaluated over several decades at the Mayo Clinic.
▪ ETIOLOGY AND PATHOGENESIS
Once considered a tuberculoid reaction, lichen nitidus is currently regarded as a disorder of unknown etiology. The relationship between lichen nitidus and lichen planus has been debated for many
years.The co-existence of both diseases in some patients and the observation that the discrete, tiny papules of lichen planus are indistinguishable from those of lichen nitidus were used to support the view that lichen nitidus is a variant of lichen planus. However, most experienced clinicians, as well as research studies, favor the separation of these two diseases as distinct entities based on both clinical and immunodermatopathologic differences and the characteristic and distinctive histologic changes.. Another etiologic theory of lichen nitidus proposes that an allergen may cause epidermal and dermal antigen-presenting cells (e.g., Langerhans cells) to activate a cell-mediated response, initiate lymphocyte accumulation, and form discrete inflammatory papules. The presence of large numbers of Langerhans cells in the infiltrate supports this theory. Specific cytokines produced by the inflammatory cells influence the immune response and may shift the T lymphocyte response toward the T helper 2 subset that has the potential to produce the superficial dermal granulomas seen in lichen nitidus.6Functional impairment in cellular immunity has been reported in generalized lichen nitidus,7 and lichenoid photoeruptions similar to lichen nitidus were seen in a patient with HIV infection. Rare cases of lichen nitidus associated with atopic dermatitis, Crohn disease, and juvenile chronic arthritis have been reported. Induction of allergic contact dermatitis by topical application of dinitrochlorobenzene in a patient with lichen nitidus cleared the eruption, presumably by altering the cellular immunity, cellular infiltration, and cytokine expression.
LICHEN NITIDUS AT A GLANCE
|
Comparison of Features between Lichen Nitidus and Lichen Planus
|
|
|
|
LICHEN NITIDUS
|
LICHEN PLANUS
|
|
Incidence
|
Rare
|
Common
|
|
Lesion
|
|
|
|
|
Size
|
Usually 1-2 mm
|
Variable, usually larger
|
|
|
Shape
|
Round
|
Polygonal
|
|
|
Color
|
Flesh, pink, red-brown
|
Erythematous to violaceous
|
|
|
Wickham striae
|
Absent
|
Present
|
|
|
Mucosal changes
|
Rare
|
Variably present
|
|
|
Pruritus
|
Uncommon
|
Usually present, marked
|
|
Histopathology
|
|
|
|
|
Hyperkeratosis
|
Variable and focal
|
Usually present
|
|
|
Parakeratosis
|
Mostly present
|
Not found
|
|
|
Infiltrate
|
Focal in one to three papillary bodies
|
Band-like, extends through many rete ridges
|
|
|
Lymphocytes
|
Variable
|
Vast majority of cells
|
|
|
Histiocytes
|
Variable, almost always present
|
Almost none
|
|
|
Giant cells
|
Occasional
|
None
|
|
|
Dyskeratotic
|
Occasional
|
Very common
|
|
Immunopathology
|
|
|
|
|
Cytoids
|
Usually negative
|
Immunoglobulin M and other conjugates
|
|
|
Basement membrane
|
Usually negative
|
Fibrinogen, other conjugates
|
|
Immunohistochemistry
|
|
|
|
|
CD4+ lymphocytes
|
Majority of cells
|
Majority of cells
|
|
|
CD68+ cells
|
Common
|
Uncommon
|
|
A rare familial presentation of lichen nitidus has been reported, although no genetic factors of the disease have been identified.9
CLINICAL FINDINGS
Lichen nitidus is composed of multiple, discrete, smooth, flat, round papules. Individual papules are 1 to 2 mm in size, flesh-colored to slightly pink or, in blacks, hypopigmented, with a glistening appearance . Sometimes, minimal scale is present or can be elicited by rubbing the surface of the papules. Occasionally, the papules are grouped and the isomorphic or Koebner phenomenon is observed. Lesions may occur anywhere over the skin surface; however, the most frequent sites of predilection are the flexural surfaces of the arms and the wrists, lower abdomen, breasts, the glans and shaft of the penis, and other areas of the genital region. Rare sites of involvement include mucous membranes, nails, palms, and soles. Rare clinical variants include vesicular, hemorrhagic, spinous follicular, linear, generalized, and actinic types.
Palmo-plantar involvement may manifest several morphologic forms. Bilateral hyperkeratosis of palms and soles with erythema, fissuring, and a texture resembling fine sandpaper has been observed. Occasionally, minute keratotic spicules on the palmar surfaces or multiple pinpoint papules that extend to the dorsa of the extremities occur . Nail abnormalities usually manifest as longitudinal, beaded ridging, and terminal splitting with or without irregular pitting. Lesions of lichen planus may infrequently be present simultaneously. Lichen nitidus is usually asymptomatic; however, pruritus is occasionally present and sometimes intense. There are no constitutional symptoms or systemic abnormalities associated with the disease. Lichen nitidus has been reported after hepatitis B vaccination.18
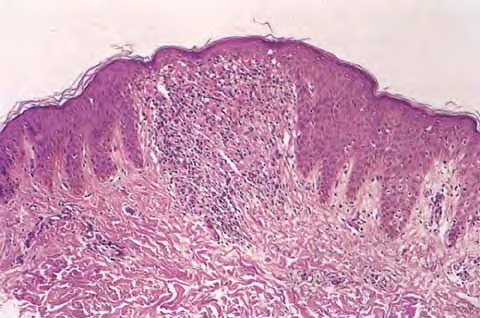
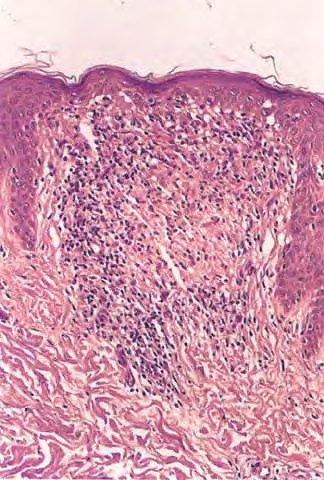
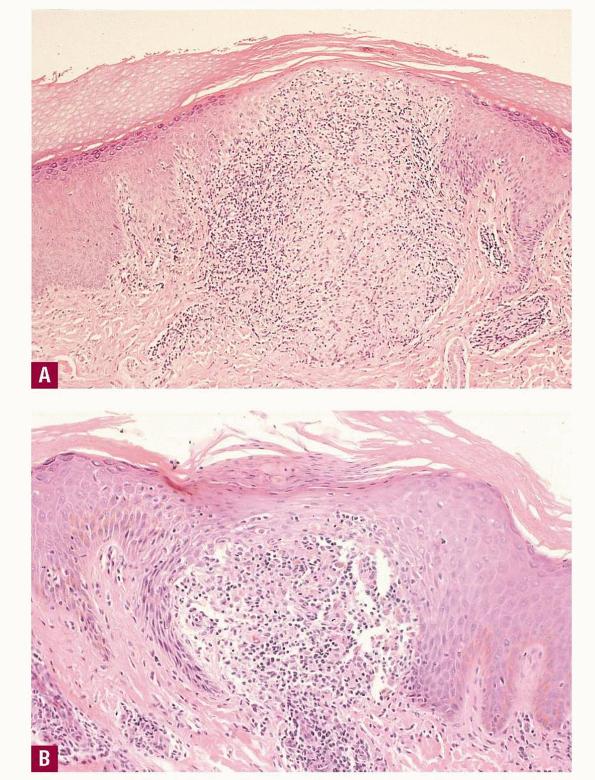
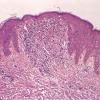
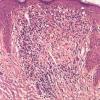
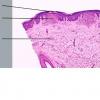
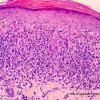
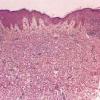
A dense mass of infiltrating lymphohistiocytic cells is situated immediately below the epidermis and results in widening of the papillary dermis with elongation and the appearance of embracement by neighboring rete ridges . Occasionally, two or three papillary spaces merge together as part of the inflammatory
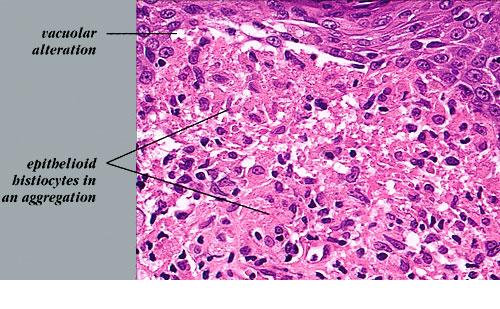
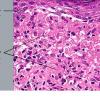
infiltrate. The overlying epidermis is thinned and occasionally demonstrates central parakeratosis without hypergranulosis. This is a characteristic diagnostic finding, when observed . Minimal hydropic degeneration with few dyskeratotic cells is usually observed within the basal epidermal layer adjacent to the papillary dermal infiltrate. With the development of hydropic degeneration, basal cell disruption, and epidermal thinning, the epidermis may partially detach from the dermis. Colloid bodies are rarely seen in lichen nitidus, in contrast to their frequent occurrence in lichen planus. The dermal infiltrate is well circumscribed and composed of closely associated histiocytes, lymphocytes, and occasional foreign body or Touton-type giant cells. Usually, no plasma cells or eosinophils are seen. In some cases, the majority of the cells in the infiltrate are histiocytic. Palmar lesions may show a deep parakeratotic plug. Transepithelial elimination of the inflammatory infiltrate has been described. Purpuric or hemorrhagic lesions are associated with capillary wall degeneration and red blood cell extravasation.11
The majority of the cells in the infiltrate are T lymphocytes intermixed
with few to many histiocyte-macrophages that stain with CD68, as well as epidermal Langerhans cells and indeterminate cells that express S100 protein. CD4+ cells predominate over CD8+ T lymphocytes. Many cells in the infiltrate express HLA-DR antigen, which implicates them as antigen-presenting cells.
Direct immunofluorescence examination of lichen nitidus is usually negative for deposition of immunoglobulins at the dermal-epidermal junction, in contrast to the vast majority (95 percent) of cases of lichen planus . Cytoids are also not usually observed in lichen nitidus. The results of ultrastructural studies coincide with light microscopic findings and also show activated lymphocyte morphology with convoluted nuclei, resembling Sézary cells.
PROGNOSIS AND CLINICAL COURSE
Lichen nitidus is typically a focal, asymptomatic, chronic inflammatory reaction that eventually resolves spontaneously after months to 1 year in two-thirds of patients or, less frequently, over a few years. Rarely, the eruption may persist indefinitely. New lesions may continue to develop as older lesions resolve. Lesions heal without scar formation or pigmentary abnormalities.
Differential Diagnosis of Lichen Nitidus
Most Likely
- o CD8 lymphocytes predominate
- o No granulomatous inflammation
- o Plaques has silvery scale
- o Variable in size
- o Verrucous surface
- o Fewer lesions than lichen nitidus
- o Less likely to involve multiple anatomic areas
- o More keratotic and scaling
- o Hand dermatitis
- o Palmo-plantar involvement of lichen nitidus
Consider
- · Lichen spinulosus
- · Papular eczema
- · Lichen scrofulosorum
- · Lichenoid syphilitic lesions
- · Bowenoid papulosis
- · Sarcoidosis
- · Lichen amyloidosus
TREATMENT
Because the disease is asymptomatic and self-limiting, no intervention is required in most cases. Treatment of lichen nitidus is warranted when it is associated with protracted pruritus or when the appearance interferes with the patient's daily activities and outlook. Topical glucocorticoids may yield favorable results. A short course of oral glucocorticoids may also be helpful and hasten resolution of more extensive, generalized, or symptomatic disease.Psoralen and ultraviolet A light, ultraviolet A and B phototherapy, astemizole, acitretin or etretinate, low-dose cyclosporine,and oral itraconazole have also been used successfully when indicated for more problematic disease.
Narrowband ultraviolet B could be a safe and effective treatment in generalized lichen nitidus. Tacrolimus ointment was also reported to be effective after 1 month of therapy.History of exposure to tuberculosis in the setting of lichen nitidus should be investigated and when appropriate treated with antituberculous medications. Complete clearance of lichen nitidus was seen in one case.