
HIDRADENITIS SUPPURATIVA
Epidemiology
Hidradenitis (HS) has a point prevalence of up to 4.1 percent based on objective findings, and a 1-year prevalence of 1 percent based on patient recall.59 This prevalence was refuted by another group of investigators, who determined a prevalence of only 1/3000. It is more common in females, with reported female-male ratios ranging from 2:1 to 5:1. The reason for female preponderance is unknown. HS rarely develops before puberty or after menopause, although persistence into menopause is not uncommon.61 The average age of onset is 23 years.62 Although the disease may develop in any apocrine gland-bearing skin, genitofemoral lesions are more prevalent in women, whereas axillary involvement does not demonstrate a gender predilection.
Etiology and Pathogenesis
Little is known about the pathogenic basis of HS. Unfortunately, only a few limited studies have attempted to clarify etiology.
More recent publications have refuted the concept that this primary event in HS is apocrine gland inflammation and postulate that apocrine glands become secondarily affected. HS is now generally considered to be a disorder of the follicular epithelium, with follicular occlusion giving rise to clinical findings. Follicular hyperkeratosis is the initial event, leading to occlusion, occasional secondary apocrine involvement, and follicular rupture with resultant inflammation and possibly secondary infection. Pathologic studies have supported this concept by demonstrating follicular obstruction, the absence of apocrine glands, and minimal or absent apocrine gland inflammation in specimens of HS.
The concept of the follicular occlusion tetrad stems from the concept that HS, acne vulgaris, pilonidal sinus, and dissecting cellulitis all share follicular occlusion as an inciting event that eventually leads to disease expression.
.
LABORATORY TESTS
Patients with acute lesions of HS may demonstrate an increase in the erythrocyte sedimentation rate or C-reactive protein. If there is any concern over infection, then deep cultures (not skin surface) from lesions should be conducted and submitted for bacterial, tuberculosis, and fungal cultures.
SPECIAL TESTS
Ultrasonography of the follicles and dermis may reveal abscess formation and abnormalities in the deep part of the follicle, but is rarely indicated. Recently, magnetic resonance imaging features of the skin and subcutaneous tissue have been described. Such features included marked thickening of the skin, induration of the subcutaneous tissues, and multiple subcutaneous abscesses.
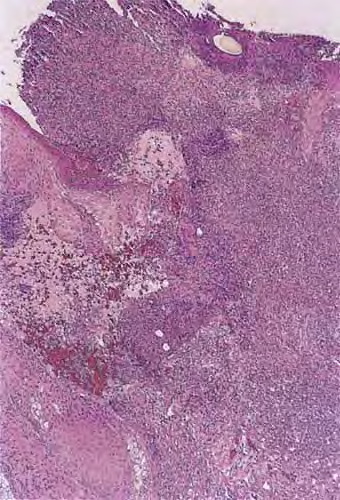
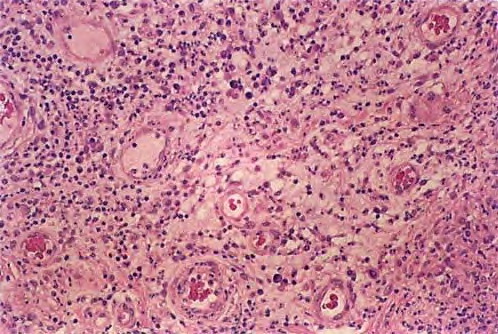
Pathology
The early lesions of HS demonstrate follicular hyperkeratosis. Other dermal features include active folliculitis or abscess, sinus tract formation, fibrosis, and granuloma formation. There is evidence of an inverse relationship between fibrosis and inflammation, supporting the concept that fibrosis corresponds to areas of chronic involvement.68 Histologic feature examination of adnexal structures reveals inflammation of the apocrine glands in only one-third of cases. Interestingly, involvement of eccrine glands (25 percent) has been reported to be more common than apocrine glands (12 percent).103,104 Poral occlusion or cyst formation may be noted. The subcutis may demonstrate some fibrosis, fat necrosis, or inflammation.
Complications
QUALITY OF LIFE
Patients with HS experience a significant degree of morbidity when quality of life is measured by the Dermatology Life Quality Index. The highest scores relate to disease-associated pain. Quality of life measurements are lower than other dermatologic diseases that have been investigated using this tool.105 Loss of workdays is a socioeconomic consequence. Women lose significantly more days of work (mean, 2.9 days) than men (mean, 1.7 days).
SYSTEMIC COMPLICATIONS
Local infection may develop and lead to septicemia. A case of lumbosacral epidural abscess has been reported.106 Anemia or leukocytosis may be detected, but does not tend to be significant clinically.
LOCAL COMPLICATIONS
Scarring may limit mobility. Anal, urethral, or rectal strictures may develop from chronic genitofemoral inflammation. Urethral fistulas have also been reported. Additionally, disfiguring persistent penile, scrotal, or vulvar lymphedema may develop,110 giving rise to significant functional impairment. This lymphedema is thought to result from fibrosis and resultant lymphatic channel obstruction. Surgical reconstruction may be necessary.111 Squamous cell carcinoma (SCC) may rarely develop in chronically inflamed and scarred areas in individuals with long-standing disease. SCC has been reported in 3.2 percent of patients with perianal HS lasting 20 to 30 years. SCC is most common in men in the anogenital region. These carcinomas tend to be more aggressive locally and are associated with a higher incidence of metastatic disease and mortality. One case of paraneoplastic neuropathy has been described in association with SCC complicating severe perineal HS.119 Clinicians should have a low threshold for biopsying any non-healing lesion localizing to an area of chronic HS. One case-controlled Swedish study found that the overall incidence of malignancy, including non-melanoma skin cancer, is increased in patients with HS.120
Treatment
The objective of patient management is prevention of the development of primary lesions as well as resolution, amelioration, or regression of secondary disease features such as scarring or sinus tract formation. The literature reveals only three randomized controlled studies, several case series, and a plethora of case reports.
MEDICAL TREATMENT
Therapy for the early stages of HS consists primarily of both topical and systemic antibiotics. Some authors advocate long-term suppressive antimicrobial therapy, although supportive evidence is lacking. Topical clindamycin has been demonstrated to be superior to placebo in a randomized clinical trial.121 A randomized controlled study comparing topical clindamycin with systemic tetracycline did not reveal a statistical difference.122
Intralesional corticosteroids may be of benefit for patients with an isolated number of tender lesions.123 Practically, such treatment may not be appropriate for individuals with extensive disease and is not appropriate for areas of chronic inflammation.
Isotretinoin as therapy for patients with HS initially held conceptual promise because both diseases share follicular occlusion in disease development. Unfortunately, isotretinoin has demonstrated only a modest therapeutic benefit. In a study of 68 patients, 23.5 percent cleared during therapy, whereas only 16.2 percent maintained improvement during a follow-up period of up to 6 months.124 One case report described an individual with severe vulvar HS who, after treatment with prednisolone and then long-term isotretinoin (more than 1 year), remained disease free at 10 months post-treatment. The other systemic retinoids, acitretin and etretinate, have also demonstrated limited efficacy in disease management.
The analogy between acne and HS has also made hormonal therapy for HS appealing. Hormonal therapy does have some reported success. In a double-blinded study, the anti-androgen, cyproterone acetate (50 mg), in conjunction with ethinyl estradiol (50 µg), resulted in complete or partial clearance at 18 months post-treatment in 50 percent of patients. The 5α-reductase inhibitor, finasteride (1 mg), may also have a weak limited effect on disease management.
Infliximab, a chimeric monoclonal antitumor necrosis factor antibody, has demonstrated efficacy in several case reports. Efficacy has been reported in two patients with Crohn disease and HS.77,129 Infliximab also was efficacious in achieving remission and controlling disease flares in an individual with HS and ulcerative colitis. Case reports or small case series have also shown therapeutic success with other systemic therapies, including systemic corticosteroids, azathioprine, cyclosporine, dapsone, and methotrexate.
Local therapies have also been recently examined. A single patient with aggressive perianal HS has responded favorably to wide surgical excision in conjunction with perilesional granulocyte-macrophage colony-stimulating factor injections.135 A small case series demonstrated the efficacy of treatment of persistent painful nodules with cryotherapy. Healing time in these patients was lengthy (18 to 42 days). Finally, the first case of botulinum toxin A successfully treating HS has been reported. In this case, injections into the axillae resulted in a 10-month remission.137
Photodynamic therapy (PDT) as treatment for HS has recently been described in two small case series. In one, four patients sustained 75 percent to 100 percent improvement over 3 months after treatment with aminolevulinic acid-PDT and blue light.138 In the other case series, three patients receiving aminolevulinic acid-PDT with either a diode
laser (633 nm) or broad band red light source (570 to 670 nm) did not experience clinical improvement.139
SURGERY
Surgical removal of all involved tissue, beyond clinically involved margins, is an effective treatment modality.140 Postoperative recurrences may occur. Some authors have advocated the use of CO2 laser for surgical ablation of tissue. The modality of closure has been a topic of debate. Overall, healing by secondary intent is thought to provide the best outcome. Primary closure, grafting, or flaps have been extensively used, but may be associated with poorer results.141-147 In one series of 106 patients, there was a 70 percent recurrence rate requiring subsequent operation in the primary closure cohort and no recurrence in the split-thickness graft and flap groups.148 A more limited surgical approach also plays a role in disease management. Deroofing or marsupializing of recurrent troublesome lesions or sinus tracts may aid with local control. Lancing an inflammatory lesion is of limited benefit and should be discouraged.
RADIOTHERAPY
Several authors have reported radiotherapy to be successful in the treatment of HS. Given the often young patient population with HS, long-term side effects must be considered