|
|
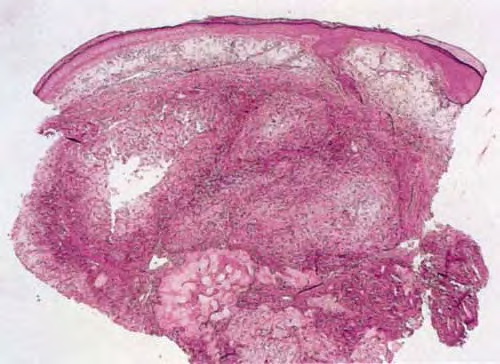
In the early stage of gout, there usually are irregularly recurring attacks of acute arthritis. In the late stage, deposits of monosodium urate form within and around various joints, leading to chronic arthritis with destruction in the joints and the adjoining bone. During this late stage, urate deposits, called tophi, may occur in the dermis and subcutaneous tissue. The incidence of tophaceous lesions in gout has significantly decreased since 1950, from 14% to 3%, even though the incidence of gout has remained unchanged. Improved methods of treatment account for this decrease
|
|
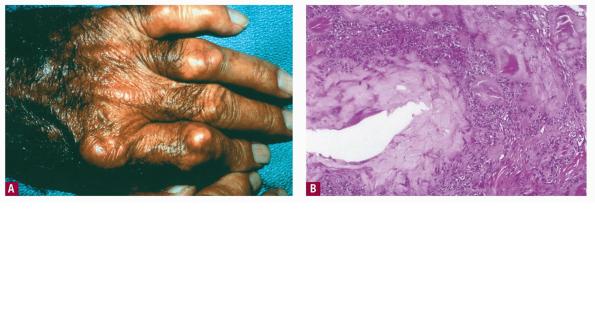
Tophi are observed most commonly on the helix of the ears, over the bursae of the elbows, and on the fingers and toes . They may attain a diameter of several centimeters. When large, tophi may discharge a chalky material. In rare instances, gout may present as tophi on the fingertips or as panniculitis on the legs without the coexistence of a gouty arthritis .
|
|
Histopathology.
For the histologic examination of tophi, fixation in absolute ethanol or an ethanol-based fixative, such as Carnoy's fluid, is preferable to fixation in formalin; it has been stated that aqueous fixatives such as formalin dissolve the characteristic urate crystals, leaving only amorphous material . However, some authors contend that formalin-fixed, paraffin-embedded tissue that is sectioned, floated in alcohol {as opposed to a water bath}, and then placed onto a slide without staining will display refractile crystals when examined under polarized light . An alternate staining protocol to preserve any urate crystals remaining in formalin-fixed tissue after processing also has been forwarded .
|
|
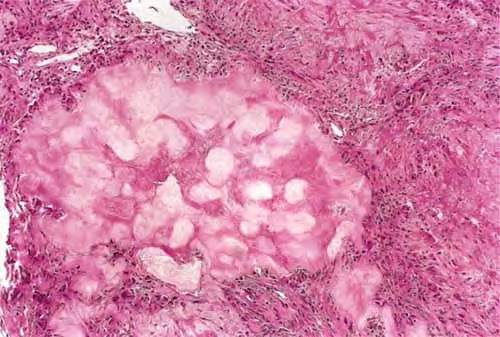
On fixation in alcohol, tophi can be seen to consist of variously sized, sharply demarcated aggregates of needleshaped urate crystals lying closely packed in the form of bundles or sheaves . The crystals often have a brownish color and are doubly refractile on polariscopic examination . If a red compensator is used along with polarizing filters in tissue that has been processed to preserve crystals, the crystals will appear yellow when they are parallel to the direction of the compensator and blue when perpendicular to it . The aggregates
|
|
Histogenesis.
Gout, a dominantly inherited disorder, is characterized by hyperuricemia. An asymptomatic stage of hyperuricemia precedes the development of gouty arthritis by many years. Patients with gout are a heterogeneous group. In some patients, diminished renal excretion of uric acid accounts for the hyperuricemia; in others, an excessive production of uric acid from increased purine biosynthesis is found. In still other patients with gout, both excessive synthesis of uric acid and decreased renal excretion of uric acid are found . The deposits of urate crystals stimulate cytokine production, chiefly interleukin-1 (IL-1). IL-1 is a central mediator of the neutrophil recruitment and activation that is characteristic of joint disease (but not a feature in dermal disease) .
|
|
of urate crystals are often surrounded by a palisaded granulomatous infiltrate containing many foreign body giant cells . The urate crystals appear black and the surrounding tissue yellow when the sections are stained with 20% silver nitrate solution .
|
|
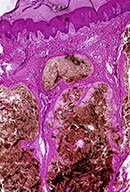
Even when the specimen has been fixed in formalin, the diagnosis of gout can be made without difficulty because of the
|
|
characteristic rim of foreign body giant cells and macrophages surrounding the aggregates of amorphous material. As a secondary phenomenon, calcification, and occasionally ossification, may take place in the sodium urate aggregates.
|
|

