Granuloma Faciale
▪ HISTORICAL ASPECTS
▪ EPIDEMIOLOGY
Granuloma faciale occurs predominantly in adult men and women. There is a slight male predominance, and mean age at presentation is 52 years. Granuloma faciale can occur in individuals of any race; however, it is more common in Caucasians. The disease presents most commonly with a single lesion on the face, but extra-facial lesions have been described. Patients with multiple lesions have also been reported. A rare mucosal variant has been described as eosinophilic angiocentric fibrosis, which typically involves the upper respiratory tract.
▪ ETIOLOGY AND PATHOGENESIS
The etiology of granuloma faciale is unknown. The disease can be considered a localized chronic fibrosing vasculitis. Immunofluorescence studies have revealed deposition of immunoglobulins and complement factors in the vessel walls consistent with a type III immunologic response, marked by deposition of circulating immune complexes in vascular lumina. However, other authors have described negative results with immunofluorescence.
▪ CLINICAL FINDINGS
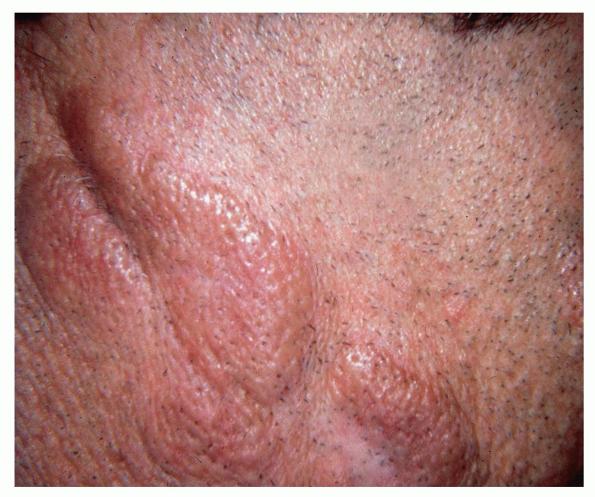
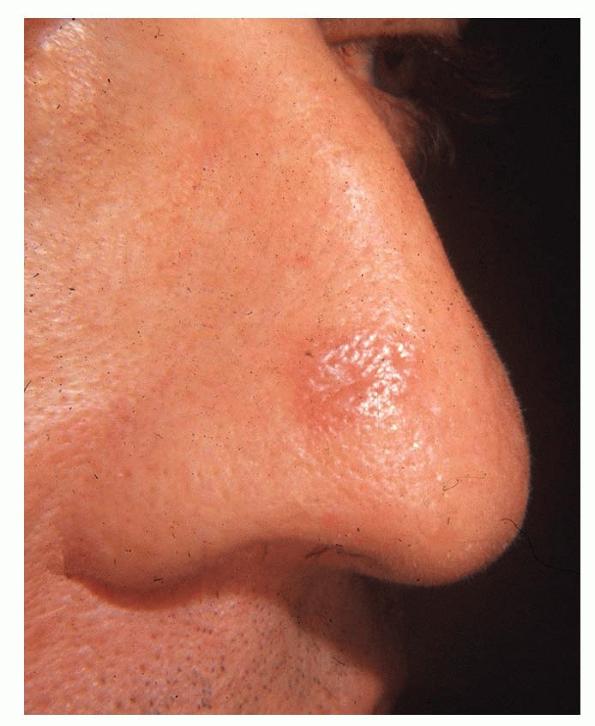
Granuloma faciale is characterized by solitary papules, plaques, or nodules. The lesions are typically asymptomatic red, brown, or violaceous plaques that are soft
and well circumscribed . Lesions are most common on the face. Sites of predilection include the nose, preauricular area, cheeks, forehead, eyelids, and ears. Rarely, patients may present with multiple lesions or lesions on the trunk or extremities. Extra-facial lesions have been reported both as isolated findings and in conjunction with facial lesions. Lesions may be present for weeks or months and tend to follow a chronic course. The plaques typically have a smooth surface and show dilated follicular ostia . Ulceration is rare. Lesions are typically asymptomatic; however, patients may complain of tenderness, burning, or pruritus.4 Photo-exacerbation of lesions has been reported.
GRANULOMA FACIALE AT A GLANCE
- Granuloma faciale is an uncommon inflammatory dermatosis characterized clinically by reddish brown papules and plaques primarily involving the face.
- The pathology shows changes of a chronic leukocytoclastic vasculitis with a mixed infiltrate containing eosinophils, extensive perivascular fibrin deposition, and dermal fibrosis.
- Etiology is unknown.
▪ LABORATORY FINDINGS
An extensive laboratory evaluation is not required. Peripheral blood eosinophilia is occasionally detected.
The diagnosis may be established by a combination of clinical findings and confirmatory tissue biopsy results. A punch biopsy that includes the full thickness of the dermis is recommended. Histologic examination shows a normal-appearing epidermis, which may be separated from the underlying inflammatory infiltrate by a narrow grenz zone . Within the dermis is a dense and diffuse infiltrate of lymphocytes, plasma cells, eosinophils, and neutrophils with evidence of leukocytoclasis . The inflammatory infiltrate surrounds the blood vessels, which show evidence of fibrin deposition. In later stages, the perivascular fibrin deposition becomes extensive and dominates the histologic picture. Deposition of hemosiderin may contribute to the brown color seen clinically. Electron microscopic studies confirm the presence of an extensive eosinophilic infiltrate with Charcot-Leyden crystals and numerous histiocytes filled with lysosomal vesicles; however, cases with few eosinophils in the infiltrate have also been described.13 Immunoglobulins, fibrin, and complement can be found deposited along the dermo-epidermal junction in a granular pattern and around blood vessels by direct immunofluorescence.10
Box 33-1 Differential Diagnosis of Granuloma Faciale
Most Likely
- Face
- Sarcoidosis
- Granuloma annulare
- Lymphocytic infiltration of Jessner
- Rosacea
- Extrafacial
- Erythema elevatum diutinum
Consider
- Face
- Discoid lupus erythematosus
- Lymphoma cutis
- Angiolymphoid hyperplasia with eosinophilia
- Tinea faciei
- Basal cell carcinoma
- Xanthogranuloma
- Mastocytoma
- Extrafacial
- Granuloma annulare
- Benign lymphocytic infiltrate of Jessner
- Fixed drug eruption
Always Rule Out
- Face
- Discoid lupus erythematosus
- Trunk
- Erythema elevatum diutinum
▪ DIFFERENTIAL DIAGNOSIS
The clinical differential diagnosis for granuloma faciale includes discoid lupus erythematosus, polymorphous light eruption, fixed drug eruption, benign lymphocytic infiltrate of Jessner, lymphoma cutis, pseudo-lymphoma, sarcoidosis, granuloma annulare, tinea faciei, insect bite reaction, xanthogranuloma, mastocytoma, basal cell carcinoma, Langerhans cell histiocytosis, and rosacea . The diagnosis can be reliably made by analysis of a punch biopsy specimen. Absence of serologic evidence of lupus erythematosus helps to differentiate these lesions from the lesions of discoid lupus erythematosus.
The primary histologic differential diagnosis is erythema elevatum diutinum (EED). Both diseases represent chronic forms of fibrosing small vessel vasculitis and may be related. However, there are several clinical and histologic differences. EED is characterized by multiple lesions, primarily located on extensor surfaces of the extremities in a symmetric acral distribution. The trunk and face are typically spared in EED. Histologically, both show a chronic fibrosing vasculitis.14 However, a grenz zone of normal collagen beneath the epidermis is not typical of EED. EED may be associated with systemic conditions, primarily monoclonal gammopathies, and shows an excellent response to dapsone.15,16 The histologic and clinical differential may also include angiolymphoid hyperplasia with eosinophilia. However, the lesions of angiolymphoid hyperplasia with eosinophilia contain blood vessels with prominent “hobnail” endothelial cells that protrude into the vascular lumina rather than perivascular fibrin deposition. One case of tinea faciei caused by Trichophyton rubrum has been described with clinical and histologic changes consistent with granuloma faciale.
Treatments for
Granuloma Faciale
|
|
TOPICAL
|
PHYSICAL
|
SYSTEMIC
|
|
First-line therapy
|
Topical corticosteroids
|
Cryotherapy
Intralesional steroids
Pulsed dye laser
|
Dapsone, 50-100 mg/day
|
|
Second-line therapy
|
Topical tacrolimus ointment
|
Surgical excision
|
|
▪ COMPLICATIONS
Granuloma faciale is rarely associated with systemic toxicity.
▪ PROGNOSIS AND CLINICAL COURSE
Lesions tend to be chronic and resistant to treatment.
▪ TREATMENT
A variety of medical and surgical therapies have been used in the treatment of granuloma faciale . Because of the small number of patients involved, randomized trials to evaluate these treatments are lacking. Resistance to therapy and cosmetic complications should be discussed with the patient before initiation of therapy. Topical and intralesional steroids have been administered with modest improvement. Cryosurgery has been applied with effective results. Because the disease is known to be a variant of chronic leukocytoclastic vasculitis, dapsone 25 to 100 mg/day has been used with benefit in a number of patients.22,23 Topical tacrolimus ointment 0.1 percent also has been used with success.
Surgical excision may be an option for small lesions. Lesions of granuloma faciale have been treated with a variety of medical lasers. In one study, the Candela Vbeam pulsed dye laser at 595 nm provided resolution in two of four patients. A variety of pulsed dye lasers have been used with similar results. A carbon dioxide laser has also been applied with varying success.30 The use of an argon laser resulted in total resolution of the granuloma faciale with subsequent scarring. The lesions in two patients were reported to respond to the Laserscope potassium-titanyl-phosphate 532-nm laser in combination with tacrolimus ointment 0.1 percent.