|
Epidermal naevus
Epidermal nevi (EN) are congenital hamartomas of embryonal ectodermal origin classified on the basis of their main component; the component may be sebaceous, apocrine, eccrine, follicular, or keratinocytic. An estimated one third of individuals with epidermal nevi have involvement of other organ systems; hence, this condition is considered to be an epidermal nevus syndrome (ENS). Solomon defines epidermal nevus syndrome as a sporadic neurocutaneous linkage of congenital ectodermal defects in the skin, brain, eyes, and/or skeleton. Epidermal nevus syndrome is often termed the Solomon syndrome. Schimmelpenning first detailed epidermal nevi with neurologic anomalies; hence, the term Schimmelpenning syndrome. The term organoid nevus may be used to emphasize the admixture of epidermal cells often evident in individual lesions of epidermal nevi.
Gustav Schimmelpenning, born in 1928 in Oldenburg (Germany), served from 1971-1994 as the head of the Department of Psychiatry at the University of Kiel.1 In 1957, he described a case of sebaceous nevus involving the head, with ipsilateral ocular lesions including coloboma of the upper lid, increased density of cranial bones, epileptic seizures, and mental retardation. He called this combination of anomalies a new phacomatosis. Subsequently, others reported this phenotype as Schimmelpenning syndrome, Feuerstein-Mims syndrome, Schimmelpenning-Feuerstein-Mims syndrome, epidermal nevus syndrome, Solomon syndrome, linear sebaceous nevus (LSN) syndrome, organoid nevus phacomatosis, or Jadassohn nevus phacomatosis.
A clinical entity called epidermal nevus syndrome should be more precisely defined and distinguished by clinical, histopathologic, and genetic criteria. In this review, 4 distinct epidermal nevus syndromes, recognizable by the different types of associated epithelial nevi, are described. These include linear sebaceous nevus, linear nevus comedonicus (NC), linear epidermal nevus (LEN), and inflammatory linear verrucous epidermal nevus (ILVEN). Each type may be regarded as part of a syndrome with systemic associations.
Linear epidermal nevus syndrome is a congenital neurocutaneous disorder characterized by linear epidermal nevus with significant involvement of the nervous, ophthalmologic, and/or skeletal systems.2 Clinical manifestations include mental retardation, seizures, and movement disorders that are caused by a wide range of neuropathologic lesions. Intracranial and/or intraspinal lipomas may occur.
Linear sebaceous nevus, also known as organoid nevus syndrome, often has the term linear deleted because almost all syndromic sebaceous nevi are linear. It has also been called Schimmelpenning-Feuerstein-Mims syndrome and Jadassohn nevus phakomatosis. Schimmelpenning syndrome, as noted above, links a sebaceous nevus with cerebral anomalies, coloboma, and lipodermoid of the conjunctiva.
Linear nevus comedonicus is also known as comedone nevus, nevus follicularis keratosus, nevus acneiformis unilateralis, and nevus zoniform. Cataracts may be a prominent feature of nevus comedonicus syndrome.
Inflammatory linear verrucous epidermal nevus is a linear, persistent, pruritic plaque, usually first noted on a limb in early childhood. Originally described by Unna in 1896, a few patients were reported prior to 1971 when Altman and Mehregan3 delineated inflammatory linear verrucous epidermal nevus as a distinct entity in 25 patients. They coined the name inflammatory linear verrucous epidermal nevus, labeling it a clinical and histopathologic type of linear verrucous nevus that is often inflammatory or psoriasiform. Inflammatory linear verrucous epidermal nevus accounts for approximately 5% of patients with epidermal nevi and has been described in a mother and daughter.
Six different syndromes with epidermal nevi as part of them have been delineated. These include (1) Proteus, (2) congenital hemidysplasia with ichthyosiform nevus and limb defect, (3) phakomatosis pigmentokeratotica, (4) sebaceous nevus, (5) Becker nevus, and (6) nevus comedonicus4 syndromes.
The spectrum has recently been expanded with the description of linear Cowden nevus as a new distinct epidermal nevus.5 This nonorganoid epidermal nevus is probably due to loss of heterozygosity, occurring at an early developmental stage in an embryo with a germline PTEN mutation, giving rise to Cowden disease.
Pathophysiology
Epidermal nevi arise from pluripotential germinative cells of the basal layer of the embryonic epidermis.
Inflammatory linear verrucous epidermal nevus is distinct from psoriasis; however, they may share some common pathogenic pathways. These pathways are probably mediated by interleukin 1, interleukin 6, tumor necrosis factor-alpha, and intercellular adhesion molecule-1.
Epidermal nevus syndrome–associated skeletal disease focal bone defects may manifest as fibrous dysplasia, even without the typical radiographic or histopathologic findings of fibrous dysplasia.6 A patient had elevated circulating fibroblast growth factor 23 (FGF-23) levels with no activating mutations. This focal skeletal disease may be a source of FGF-23 in persons with epidermal nevus syndrome and thus may be a clue to its pathogenesis.
A bilateral, systematized epidermal nevus syndrome patient was described with cerebral involvement caused by a mosaic FGFR3 mutation, possibly representing a distinct entity within the group of epidermal nevus syndromes.
History
Epidermal nevi are patches, plaques, or nodules that may be bilateral or distributed on most of the body. Usually, no symptoms of the nevi are present, with the exception of inflammatory linear verrucous epidermal nevus.
Inflammatory linear verrucous epidermal nevus is a linear, persistent, pruritic plaque, usually first noted on a limb in early childhood. The clinical history may reflect symptoms associated with underlying anomalies. Inflammatory linear verrucous epidermal nevus, unlike the other types of epidermal nevi, demonstrates erythema and sometimes pruritus.
Physical
Linear nevus comedonicus
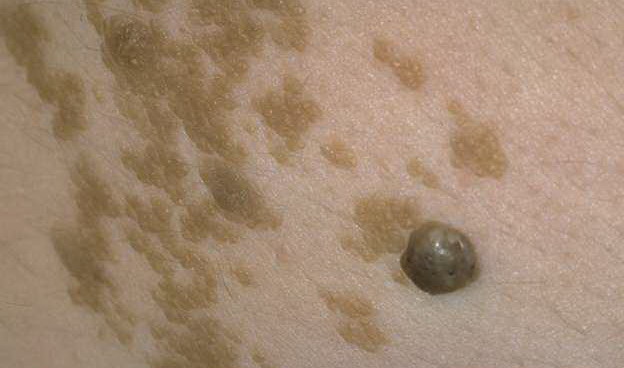
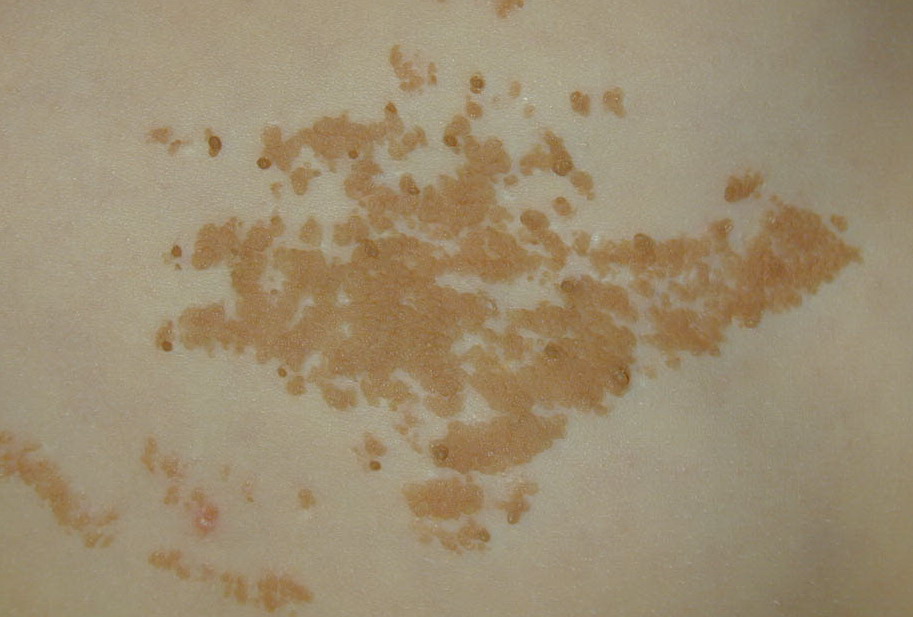
Nevus comedonicus is evident clinically as confluent clusters of dilated follicular orifices plugged with keratin, giving the appearance of aggregated open comedones. These clusters are often arranged in a linear or zosteriform pattern, occasionally paralleling the lines of Voigt or the lines of Blaschko.
Although usually unilateral, bilateral occurrences have been noted. As with other epidermal nevi, the most common sites are the face, the trunk, and proximal extremities.
Nevus comedonicus may be associated with a number of other cutaneous and internal defects, such as skeletal anomalies (eg, scoliosis, fused vertebrae or hemivertebrae, spina bifida occulta, absent fifth finger), central nervous system defects (eg, seizures, changes noted on EEG, transverse myelitis), and ocular alterations (eg, cataracts).
Inflammatory linear verrucous epidermal nevus
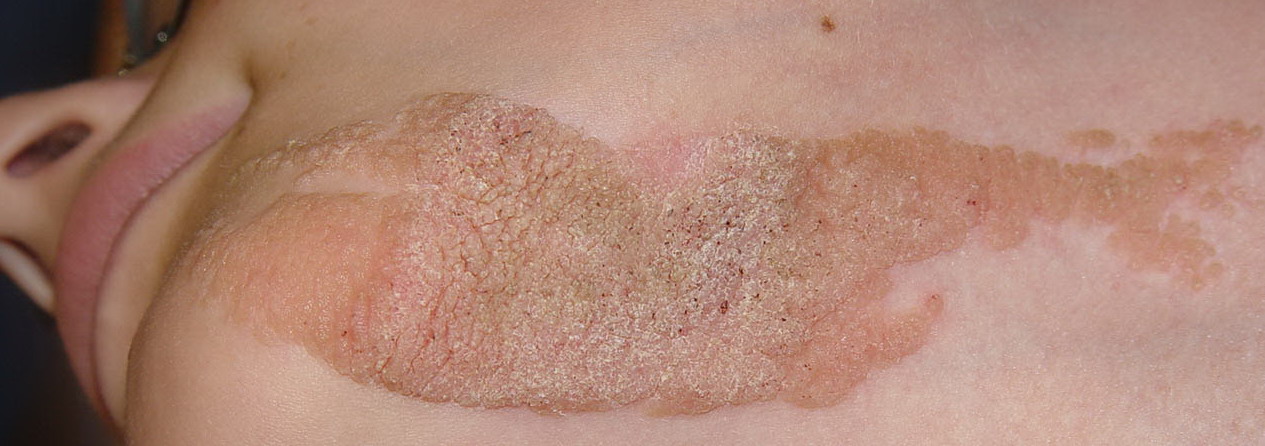
Inflammatory linear verrucous epidermal nevus is a linear, persistent, pruritic plaque, usually first noted on a limb in early childhood. Inflammatory linear verrucous epidermal nevus is characterized by tiny, discrete, erythematous, slightly warty papules, which tend to coalesce in a linear formation.
Altman and Mehregan3 delineated 6 characteristic features: early age at onset, predominance in females (with a female-to-male ratio of 4:1), frequent involvement of the left leg, pruritus, marked refractoriness to therapy, and a distinctive psoriasiform and inflammatory histologic appearance.
The lesions may be observed at birth, but most appear during infancy and childhood. In the study by Altman and Mehregan,3 one half of patients were noted to have lesions by age 6 months with three quarters of the 25 patients developing lesions by age 5 years. Several patients were noted to develop lesions at an older age (eg, 1 patient developed a lesion at 49 y). The left side of the body, particularly on the left lower extremity, was more often involved.
Inflammatory linear verrucous epidermal nevus may occur with musculoskeletal abnormalities in a few children, prompting the classification of inflammatory linear verrucous epidermal nevus as part of epidermal nevus syndrome. One infant had inflammatory linear verrucous epidermal nevus with congenital dislocation of the ipsilateral hip and Fallot tetralogy of the heart. Another infant had congenital inflammatory linear verrucous epidermal nevus with congenital bony anomalies of the ipsilateral extremities. Nevus depigmentosus and inflammatory linear verrucous epidermal nevus may occur together, as may inflammatory linear verrucous epidermal nevus and melanodontia.
Linear sebaceous nevus (Jadassohn nevus phacomatosis)
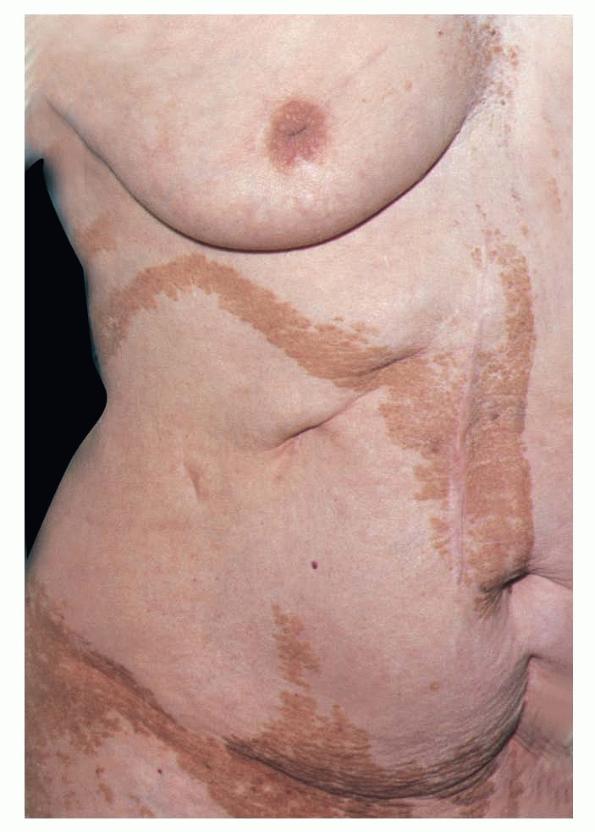
In 84% of patients with linear sebaceous nevus, skin lesions are on the face, and in approximately 50%, lesions are on the scalp, the neck, and the forehead. In most patients, the lesions appear on 1 side of the body (nevus unius lateralis), as shown in the images below. Lesions on the scalp are devoid of hair
Seizures are reported in 75% of patients with linear sebaceous nevus, mostly appearing in the first 6 months of life. The morphology of the seizures varies from infantile spasms or focal motor seizures to generalized tonic or tonic-clonic seizures. In some children, seizures are drug resistant and may result in progressive mental retardation, which is noted in approximately 70% of patients with Jadassohn nevus phacomatosis. Such regression of mental capacity is not observed in older children or adolescents.
Approximately 50% of patients demonstrate different neurologic deficits, including cranial nerve paresis (cranial nerves VI and VII), hemiparesis, or cortical blindness.
Linear sebaceous nevus syndrome is composed of multiple, well-demarcated linear, hairless plaques with evidence of neurologic or skeletal alterations, such as epilepsy or mental retardation. Skin lesions in linear sebaceous nevus syndrome are less obvious in infancy, and they are a smooth yellow-orange plaque. The nevus distribution pattern in this Schimmelpenning syndrome usually follows the lines of Blaschko. With age, these lesions become more visible, darker, verrucous, and hyperkeratotic. The last stage of development occurs in late adolescence or early adult life. The verrucous nature of the lesions is further emphasized with cutaneous benign or malignant neoplasms noted in as many as 20-30% of patients. Syringocystadenoma papilliferum is the most likely benign neoplasm, whereas basal cell carcinoma, squamous cell carcinoma, and keratoacanthoma are the most common in the malignant category
Epidermal nevus syndrome has been described in association with a complex ocular choristoma.10 Further experience may show whether this linkage is significant.
Linear epidermal nevus may be bilateral or distributed on most of the body. The lesions appear as asymptomatic patches or plaques, with the head and the neck, as well as the trunk, being the most common sites.
The lesions may have a somewhat verrucous appearance. They lack erythema, and they are not pruritic.
An epidermal nevus may be associated with oral involvement and cleft palate.11
Epidermal nevus syndrome has been described with a combination of widespread eccrine proliferation, multiple facial and oral poxlike lesions, gingival synechiae, blepharophimosis, body asymmetry, and mental retardation. This complex phenotype fits the genetic mosaicism theory.12
Causes
The basis of the cause may be the activation of an autosomal dominant lethal mutation that survives by mosaicism. These cells might survive only by being adjacent to normal ones13 Inflammatory linear verrucous epidermal nevus has been described in a mother and daughter.
Other Problems to Be Considered
The ichthyosiform nevus of CHILD syndrome (congenital hemidysplasia with ichthyosiform erythroderma and limb defects syndrome) resembles inflammatory linear verrucous epidermal nevus, but CHILD syndrome has yellowish waxy scaling and histologic features of a verruciform xanthoma. Linear psoriasis with papules in a linear configuration may represent a Koebner reaction. Linear psoriasis is distinct from inflammatory linear verrucous epidermal nevus because linear psoriasis develops either later in life in patients with plaque-type psoriasis or as congenital plaque-type psoriasis with subsequent linear distribution along the lines of Blaschko. Inflammatory linear verrucous epidermal nevus and psoriasis each have a different protein analysis and a different pattern of epidermal keratin 16 and keratin 10 expression.
Other linear eruptions may clinically resemble inflammatory linear verrucous epidermal nevus and linear epidermal nevus; however, their histologic findings usually distinguish them. Lichen striatus (LS) tends to occur in children rather than in adults. LS consists of discrete erythematous, scaly, flat-topped asymptomatic papules on 1 of the extremities. LS has a sudden onset and spontaneous regression within 1 year.
Linear lichen planus typically occurs in children, in whom the characteristic discrete pruritic polygonal violaceous papules are arranged in a linear fashion, usually extending along an entire limb. Linear porokeratosis is a childhood disorder characterized by small, ringlike, hypertrophic verrucous plaques with a linear morphology usually limited to a single extremity. At times, linear lichen simplex chronicus, linear Darier disease, linear lichen nitidus, and linear human papillomavirus–induced warts may require differentiation from linear epidermal nevus and inflammatory linear verrucous epidermal nevus.
Linear epidermal nevus in the genital area may be mistaken for genital warts.14
Trichoblastomas with Merkel cell proliferation in nevi sebacea in Schimmelpenning-Feuerstein-Mims syndrome may facilitate histological differentiation between trichoblastomas and basal cell carcinomas.15 The detection of multiple Merkel cells within the epidermal layer by cytokeratin 20 staining was considered to be an important clue.
Workup
Imaging Studies
MRIs can be used to evaluate intracranial involvement. MRIs may show cerebral atrophy, dilated ventricles, hemimegalencephaly, pachygyria, or enlarged white matter.
Multiple abnormalities are found on neuroimaging studies in patients with Jadassohn nevus phacomatosis. Findings include hemimegalencephaly (usually ipsilateral to the major skin lesions and contralateral to neurologic deficits), cortical atrophy, pachygyria, cortical heterotopias, agenesis of the corpus callosum, and Dandy-Walker syndrome.
Other Tests
EEG findings are abnormal in approximately 90% of patients. In almost all patients who had focal paroxysmal electroencephalographic abnormalities, the epileptiform focus was ipsilateral to the major skin lesions.
Histologic Findings
Histologic examination of the 4 types of epidermal nevi is variable.
Typically, the histologic examination of linear epidermal nevus reveals marked hyperkeratosis, papillomatosis, and acanthosis with rete ridge elongation in a psoriasiform pattern. Changes of epidermolytic hyperkeratosis, acantholytic dyskeratosis, and those resembling verruca vulgaris and comedo formation may also be observed.
Histologic examination of inflammatory linear verrucous epidermal nevus reveals a similar psoriasiform hyperplasia of the epidermis, alternating parakeratosis without a granular layer, and orthokeratosis with a thickened granular layer. Occasionally, changes of epidermolytic hyperkeratosis, acantholytic dyskeratosis, and those resembling verruca vulgaris and comedo formation may be noted.
In nevus comedonicus, rudimentary hair follicles are dilated to form epidermal invaginations, which are filled with keratin in concentric lamellae. The follicular walls are composed of several layers of keratinocytes, which occasionally show changes of epidermolytic hyperkeratosis. Scattered hair shafts and small sebaceous lobes may be evident in early specimens; in older specimens, the shafts and lobes, as well as arrector pili muscles, are absent. The interfollicular epidermis is often papillomatous and hyperkeratotic, and ossification may be observed in the dermis.
Linear sebaceous nevus combines epidermal, follicular, sebaceous, and apocrine gland abnormalities. It reflects the normal sebaceous elements seen in infancy, childhood, and adolescence. Thus, in early life, the lesions are well developed because of maternal hormonal expression, whereas, in childhood, they are underdeveloped and reduced in size and number. At this stage, incomplete and undifferentiated hair structures may be a key to diagnosis, with prominent keratin-filled infundibula and malformed hair germs.
At puberty, this neoplasm tends to blossom with large, maturing sebaceous glands and papillomatous hyperplasia. In adulthood, benign appendageal tumors as well as malignant ones may develop. Syringocystadenoma papilliferum, chondroid syringoma, and nodular hidradenoma are most common in infancy. Basal cell carcinoma, squamous cell carcinoma, or keratoacanthoma are most common in adulthood. Rarely, tumors, such as apocrine carcinoma and porocarcinoma, may appear with more metastatic potential.
One series of 155 cases of linear sebaceous nevus with clinicopathologic correlation could not identify any cases of authentic basal cell carcinoma or other malignancies, whereas several examples of primitive follicular induction and trichoblastomas were evident.16 Other cutaneous hamartomas, hyperplasias, and neoplasms in that series included sebomatricoma, apocrine gland cyst, poroma, and different histopathologic variants of what are often considered to be warts (eg, classic warts, tricholemmoma, desmoplastic tricholemmoma).
Neuropathologic findings may also be evident. Nervous system changes may also occur in patients with linear epidermal nevus syndrome. Disorganization of cortical neuronal migration and organization, polymicrogyria, heterotopia, white matter gliosis, increased neuronal size, and/or excessive neuron and astrocyte proliferation may be observed.
Medical Care
Therapy is often challenging. Epidermal nevi are usually resistant to topical and intralesional steroids, dithranol, topical retinoids, and cryosurgery. Topical calcipotriol may be effective. In the United States, calcipotriol is not approved for children younger than 12 years.17,18
For Schimmelpenning syndrome, antiepileptic medications (if needed) should be promptly considered.
Surgical Care
If the size and the site are suitable, the nevus may be excised if desired by the patient.19
A neonate with seizures, linear sebaceous nevus syndrome, and hemimegalencephaly benefited from a hemispherectomy at 36 weeks' gestational age.20
Consultations
For nevus comedonicus syndrome, if an associated cataract is present, consult an ophthalmologist for therapy.
Medication
No ideal medical therapy for the cutaneous lesions of epidermal nevus syndrome exists. The vitamin D analogue calcipotriol may be tried in each form of this disease, particularly inflammatory linear verrucous epidermal nevus.
Vitamin D analogues
May work by inhibiting epidermal proliferation, promoting keratinocyte differentiation, and/or exerting immunosuppressive effects on lymphoid cells.
Calcipotriol (Dovonex)
Synthetic vitamin D-3 analog that regulates skin cell production and development. Inhibits epidermal proliferation, promotes keratinocyte differentiation, and has immunosuppressive effects on lymphoid cells. Use 0.005% topical ointment.
Adult
Apply a thin film to affected skin qd/bid to response
Pediatric
Administer as in adults
.
|

