Acrokeratosis Verruciformis Hopf
Acrokeratosis verruciformis is a rare genodermatosis with an autosomal dominant mode of inheritance. Acrokeratosis verruciformis is a disorder of keratinization characterized by multiple flat-topped, skin-colored keratotic lesions resembling plane warts typically observed on the dorsum of the hands and feet. Hopf first suggested the name acrokeratosis verruciformis in 1931.1 In 1947, Niedleman first published the largest series describing an Italian American family in which acrokeratosis verruciformis of Hopf occurred in 14 members. In the follow-up study in 1962, Niedleman and McKusick further described 24 cases in 4 generations of the same family.2 The number and distribution of cases in the latter report suggested an autosomal dominant mode of transmission.
Lesions identical to those of acrokeratosis verruciformis are also observed in many patients with acral Darier disease (also termed keratosis follicularis) or even in relatives of individuals with Darier disease. Considerable controversy surrounds the nature and relationship of acrokeratosis and Darier disease and whether they are manifestations of one genetic abnormality. Some authors suggest that acrokeratosis verruciformis of Hopf and Darier disease are distinct entities, while others maintain that they are variable expressions of the same disease, with the former being a mild expression or a forme fruste of the latter.3,4
Darier disease (keratosis follicularis) is the most important disorder to be distinguished from acrokeratosis. Darier disease, acrokeratosis verruciformis, epidermodysplasia verruciformis, plane warts, and seborrheic keratoses can be differentiated on the basis of histologic examination findings from biopsy samples from individual lesions. The hard nevus of Unna can be differentiated clinically on the basis of its late onset.4
Pathophysiology
Acrokeratosis verruciformis is has an autosomal dominant mode of inheritance. The close clinical and histological similarity of acrokeratosis verruciformis of Hopf to the acral lesions of keratosis follicularis (Darier disease) has been noted by Hopf and Darier themselves. The similarities led later observers to postulate a relationship between the 2 diseases. The exact relationship between acrokeratosis verruciformis and Darier disease is still controversial. A classic case of Darier disease poses no diagnostic problem. However, deciding whether a mild case of Darier disease represents, in fact, acrokeratosis verruciformis, remains difficult.
Although clinically similar, acrokeratosis verruciformis is thought to remain nondyskeratotic and nonacantholytic throughout life, whereas acral lesions of Darier disease show, upon careful histologic examination, various gradations of acantholytic dyskeratosis, especially in older lesions. Basically, the keratinization process in acrokeratosis verruciformis is exaggerated but normal, whereas in Darier disease, it is accentuated, altered, and faulty.3
A mutation in ATP2A2, a gene situated on band 12q23-q24 encoding for sarco(endo)plasmic reticulum Ca2+ ATPase2 (SERCA2), is the cause of Darier disease.5 SERCA2 is a calcium pump of sarcoplasmic/endoplasmic reticulum that plays a role in intracellular signaling. Considering the possible relationship between the 2 diseases, one report has shown that acrokeratosis verruciformis can arise from a missense mutation in ATP2A2.6 This finding suggests that the 2 diseases are allelic disorders with phenotypic expression of different severities. A more recent study provides evidence for genetic heterogeneity of acrokeratosis verruciformis and demonstrates that mutations in genes other than ATP2A2 are responsible for acrokeratosis verruciformis in some patients.7
History
- Acrokeratosis verruciformis is usually present at birth or manifests in early childhood, but the onset may be delayed until the fifth decade of life.
- Acrokeratosis verruciformis of Hopf has an autosomal dominant mode of transmission, but sporadic cases also occur.8
Physical
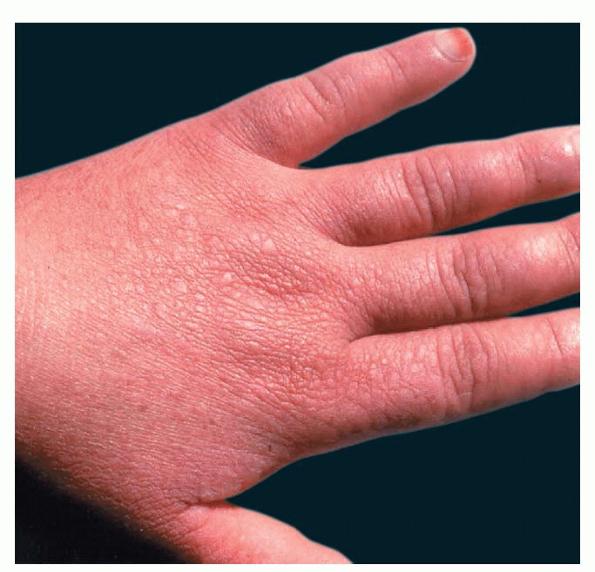
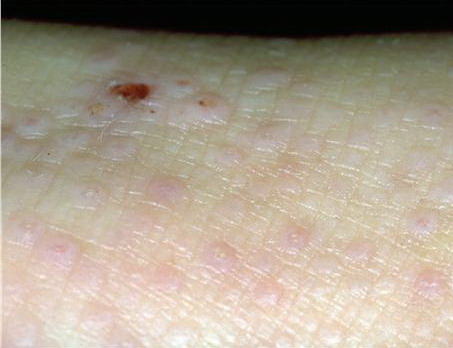
- Dry, rough, skin-colored or reddish-brown, flat-topped, or warty papules resembling flat warts are observed, particularly on the dorsum of the hands and, at times, on the dorsum of the feet.
- Papules also may be found on the knees, elbows, forearms, or lower legs.
- Small groups or isolated papules may develop on other parts of the body.
- Papules sometimes are more easily felt than seen.
- Palmar skin may be thickened and may show punctate keratosis or punctiform breaks in dermatoglyphics, identical to those observed in persons with Darier disease or Grover disease.9
- Nail involvement, including longitudinal splitting, striations, and subungual hyperkeratosis, also may be seen.10
Causes
- Acrokeratosis verruciformis of Hopf has an autosomal dominant mode of transmission. This has been suggested since 1962, in a large follow-up series by Niedleman and McKusick that described 24 cases in 4 generations in the same family.2
- Sporadic cases can also occur.8
- Acrokeratosis verruciformis and Darier disease are allelic disorders. ATP2A2 encoding the SERCA2 pump has been identified as the defective gene in Darier disease. In 2003, Dhitavat et al identified a heterozygous P602L mutation in the ATP2A2 gene in a family affected with acrokeratosis verruciformis for 6 generations.6 This mutation predicts a nonconservative amino acid substitution in the ATP-binding domain of the molecule. The mutation segregates with the disease phenotype in the family and was not found in 50 controls. Moreover, functional analysis of the P602L mutant showed that it has lost its ability to transport Ca2+. This result demonstrates loss of function of the SERCA2 mutant in acrokeratosis verruciformis, thus providing evidence that acrokeratosis verruciformis and Darier disease are allelic disorders.
- Exceptionally, a similar association with Hailey-Hailey disease has been reported.11
- Acrokeratosis verruciformis of Hopf has been reported in a patient with nevoid basal cell carcinoma syndrome.12
- The possible occurrence of squamous cell carcinoma in the context of the lesions of acrokeratosis verruciformis of Hopf has been rarely described, and one case report describes an association with keratoacanthomas.13,14
- This condition may also be associated with hypertrophic lichen planus and multiple steatocystomas.1
Histologic Findings
The sections reveal hyperkeratosis, regular acanthosis, and papillomatosis with a prominent granular layer, typically having a “church spire” appearance. Parakeratosis is not a feature. No epidermal vacuolization is present, and a mild dermal inflammatory infiltrate can be seen.8
Darier disease is the most important differential diagnosis, and patients may show identical findings upon clinical examination. Dyskeratotic cells are characteristic of Darier disease, especially in well-established lesions, but these are not present upon histologic examination of acrokeratosis verruciformis.
Epidermodysplasia verruciformis, plane warts, and seborrheic keratoses, which may also clinically simulate lesions of acrokeratosis verruciformis, can be distinguished on the basis of histologic features
Medical Care
The only effective treatment is superficial ablation. Treatment is not generally recommended, but medical and surgical treatments have been tried.17 Applications of retinoic acid have been helpful in some individuals. Destruction of the lesions with cryotherapy or laser, especially destructive lasers such as a carbon dioxide or Nd:YAG laser, may be used. Untreated lesions persist and become more noticeable after prolonged sun exposure because of darkening.
Medication
Tretinoin has been reported to be successful in some individuals with these lesions. Additionally, in a reported case of acrokeratosis verruciformis of Hopf associated with keratoacanthomas, treatment with acitretin dramatically improved both conditions.14
Retinoids
Tretinoin (Avita, Retin-A)
Developed to treat acne vulgaris. Alters maturation and differentiation of keratinocytes. Has been used for a variety of conditions, including flat warts, abnormalities of keratinization, and other keratoses.
Available in 0.025%, 0.05%, and 0.1% concentrations in a variety of vehicles, including gels, solutions, and creams.
Adult
Begin with lowest tretinoin formulation and increase as tolerated; apply hs or qod; lower frequency of application if irritation develops
Pediatric
<12 years: Not established
>12 years: Administer as in adults
.