ZINC
Zinc is an important micronutrient that is an essential component of many metalloenzymes involved in a variety of metabolic pathways and cellular functions, and is particularly important in protein and nucleic acid synthesis. Adequate zinc levels are also important for wound healing and for T-cell, neutrophil, and natural killer cell function. Zinc homeostasis depends on adequate zinc absorption and maintenance of appropriate intracellular and extracellular zinc levels. Dietary sources of zinc include meat, fish, shellfish, eggs, dairy products, and legumes, with the highest and most bioavailable forms of zinc found in meats, fish, and shellfish. Other vegetables, fruits, and refined carbohydrates contain very little zinc. Phytates (found in cereal grains, legumes, and nuts) and fiber interfere with intestinal zinc absorption. Human breast milk contains very high levels of zinc during the first 1 to 2 months of lactation, averaging 3 mg/L; subsequently, zinc levels decrease. Human breast milk also contains a zinc-binding ligand that increases the bioavailability of breast milk zinc. Although cow's milk formula contains higher levels of zinc, the bioavailability is significantly less than that in human breast milk.
Enteral zinc absorption occurs in the small intestine. Zinc excretion occurs primarily via the gastrointestinal tract via pancreatic and intestinal secretions, with lesser amounts excreted in the urine complexed to free amino acids. Two important families of zinc transporter proteins, including 9 ZnT (zinc transporter) genes and 15 Zip (Zrt- and Irt-like proteins) transporters, have been identified in humans.
Although total body zinc is stored primarily in the bones, muscles, prostate, and skin, there is no free exchange of stored zinc, and metabolic needs must be met by a continued supply of dietary zinc. In plasma, approximately 50 percent of the total zinc is complexed with albumin, while the remainder is bound to other serum proteins, including transferrin and α2-macroglobulin, or bound to free amino acids. Plasma levels may decrease transiently in response to intercurrent illness, surgery, or other stressors. Excess plasma zinc levels inhibit copper absorption, possibly through competitive inhibition of a common divalent cationic transporter. Zinc deficiency also results in impaired mobilization of hepatic retinol stores and is associated with impaired night vision (nyctalopia). Conversely, excessive calcium intake can interfere with normal zinc absorption, likely also a result of competitive inhibition.
Zinc Deficiency.
EPIDEMIOLOGY.
Zinc deficiency occurs worldwide. Populations at special risk include patients with intestinal malabsorption syndromes, liver disease, anorexia nervosa or food faddism, extensive cutaneous burns, and nephrotic syndrome. Iatrogenic zinc deficiency may result from prolonged parenteral or enteral nutrition that contains inadequate zinc levels to meet metabolic demands. Certain rural populations with diets high in phytates, as have been reported in certain parts of Iran, Turkey, and Yugoslavia, are also at risk for acquired zinc deficiency.
ETIOLOGY AND PATHOGENESIS.
Zinc deficiency may be either inherited or acquired. The inherited form of zinc deficiency, AE, classically presents during infancy on weaning from breast milk to formula or cereal, which have lower zinc bioavailability than breast milk. These infants have a defect in an intestinal zinc transporter, the human ZIP4 protein, which prevents appropriate enteral zinc absorption.87, 88, 89 There is a form of acquired zinc deficiency that may also present during infancy but, in contrast to AE, these infants become symptomatic while breast-feeding and improve after weaning to formula or table foods. Many of these reported infants have been premature, but cases have also been reported in full-term infants. The mothers of these infants have a presumed defect in mammary excretion of zinc into their breast milk, resulting in inadequate zinc intake in their infants.90-92 Measurement of breast milk zinc levels is diagnostic when less than 70 µg/dL.
Acquired zinc deficiency may result from states associated with inadequate intake, impaired absorption, or increased excretion, including pregnancy, lactation, extensive cutaneous burns, generalized exfoliative dermatoses, food faddism, parenteral nutrition, anorexia nervosa, and even excessive sweating. Intestinal malabsorption syndromes, such as inflammatory bowel disease and cystic fibrosis, result in impaired intestinal absorption of zinc, whereas alcoholism and nephrotic syndrome result in increased renal zinc losses. Penicillamine has been reported to cause zinc deficiency in a patient with Wilson disease. Ornithine transcarbamylase deficiency has also been associated with zinc deficiency.
CLINICAL FINDINGS.
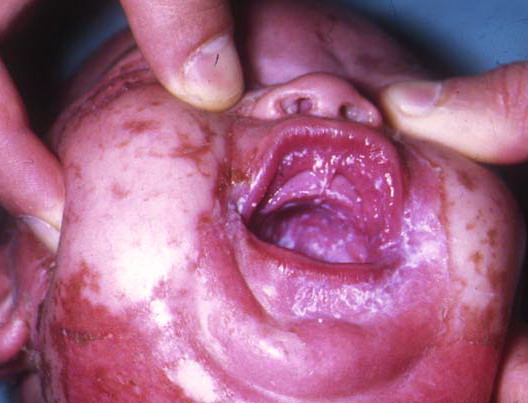
AE presents soon after weaning in affected infants or during the fourth to tenth week of life in infants who are not breast-fed. The classic features of AE include alopecia, diarrhea, lethargy, and an acute eczematous and erosive dermatitis favoring acral areas—perioral, periocular, anogenital, hands, and feet . The cutaneous findings are highly characteristic and often present initially as a non-specific, acrally distributed, symmetric, eczematous dermatitis. Over time, bullae and erosions with a characteristic peripheral crusted border develop. Patients also appear to be predisposed to systemic infections as a result of impaired cell-mediated immunity, and superinfection with Candida albicans and bacteria, usually Staphylococcus aureus, is common. Delayed wound healing, acute paronychia, conjunctivitis, blepharitis, and photophobia may also be observed. Diarrhea may be prominent but is not seen in all cases. If untreated, the disease is fatal. Acute zinc deficiency secondary to impaired absorption of zinc, inadequate intake, or excessive renal or intestinal losses may result in a clinical picture that resembles AE and occurs also in adults .
A chronic or subacute form of zinc deficiency is also recognized. These patients often have zinc levels in the mildly deficient range (40 to 60 µg/dL). Clinical manifestations include growth retardation in children and adolescents, hypogonadism in males, dysgeusia, poor appetite, poor wound healing, abnormal dark adaptation, and impaired
mentation. Cutaneous manifestations, when present, are usually less striking and present predominantly as a psoriasiform dermatitis involving the hands and feet and, occasionally, the knees.
LABORATORY TESTING.
A low plasma zinc level is the gold standard for diagnosing zinc deficiency. Use of contaminated needles, catheters, and sample tubes may lead to erroneously high measured zinc levels. Contact with collection tubes with rubber stoppers should be avoided as they may contain high levels of zinc. Hemolyzed samples are also inaccurate, as red blood cells contain very high zinc levels and cell lysis releases zinc. Normal plasma zinc levels range from 70 to 250 µg/dL. Measurement of serum AP—a zinc-dependent enzyme—is another useful indicator of zinc status, as AP may be low even when plasma zinc levels are lownormal; serum AP will increase with zinc supplementation, thus confirming the diagnosis.
In cases in which the plasma zinc level is equivocal and the diagnosis is uncertain, skin biopsy for routine histology may be helpful. The characteristic features are variable psoriasiform hyperplasia with confluent parakeratosis, spongiosis and pallor of the upper epidermis, focal dyskeratosis, and variable epidermal atrophy, These findings, however, are not specific; any may be seen in a number of other nutritional deficiencies.
TREATMENT.
Zinc supplementation with either an enteral or parenteral formulation is appropriate. Clinical response is usually rapid, with initial improvement noted within several days. Although several zinc formulations are available, the most commonly used enteral formulation is zinc sulfate. Zinc chloride is recommended for parenteral supplementation.
In children, 0.5 to 1.0 mg/kg of elemental zinc given as one to two daily doses is recommended for mild to moderate zinc deficiency. Higher doses may be required in cases of acquired zinc deficiency due to intestinal malabsorption. In adults, 15 to 30 mg of elemental zinc per day is usually sufficient in cases of acquired zinc deficiency. Serum zinc levels should be monitored during therapy. Patients with AE require lifelong treatment. Patients with acquired zinc deficiency may need variable levels of supplementation, depending on their underlying disease. Of note, excess zinc levels may interfere with copper metabolism.
Zinc Toxicity.
Zinc toxicity has been reported with exposure to zinc-containing fumes, intravenous poisoning, and ingestion of large amounts of zinc. There are no cutaneous manifestations. Severe vomiting, nausea, lethargy, dizziness, neuropathy, and dehydration. Hypocupremia may result