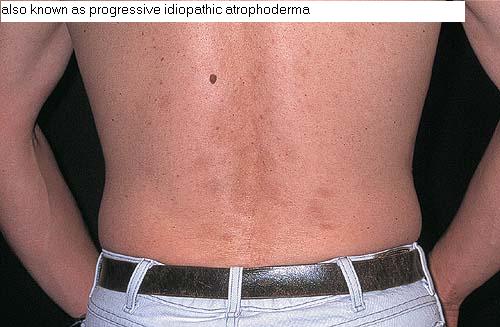
Idiopathic
Atrophoderma of
Pasini and Pierini
EPIDEMIOLOGY AND
PATHOGENESIS
Idiopathic atrophoderma of Pasini and Pierini is a form of dermal atrophy that presents as one or several sharply demarcated depressed patches with no outpouching, usually on the back of adolescents or young adults. Whether atrophoderma is a nonsclerotic, primarily atrophic variant of morphea or a separate distinct entity is still debated. Its relationship to morphea is favored by its striking clinical and histologic similarities to the atrophy seen at sites of regressing plaques of morphea. Antibodies to Borrelia burgdorferi have been reported. Typical lesions of morphea, lichen sclerosus, and atrophoderma have been observed to occur simultaneously in the same patient but in different areas, supporting the view that these conditions are related. In a series of 139 patients, 17 percent had white induration in the central portions of their atrophic lesions, and 22 percent had superficial plaques of morphea co-existing in areas outside of their atrophic foci. However, to some, the different course and outcome of atrophoderma of Pierini and Pasini as compared with morphea justifies preservation of a distinct name.
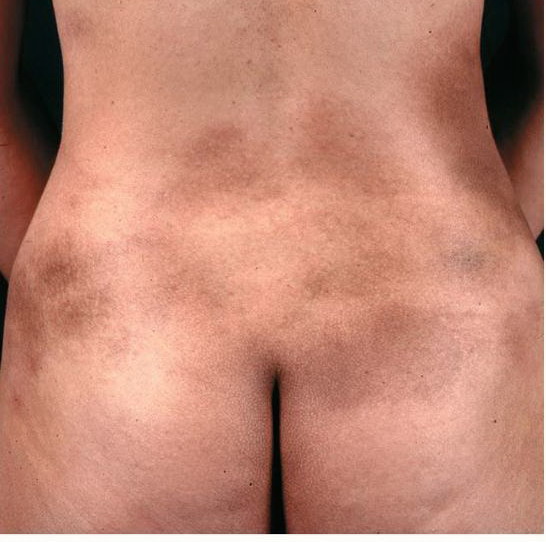
This disorder is more frequently encountered in women than in men, with a ratio of 6:1. It usually starts insidiously in young individuals in the second or third decades of life. The lesions usually occur on the trunk, especially on the back and lumbosacral region, followed in frequency by the chest, arms, and abdomen. The distribution is often symmetric and bilateral.
The lesions are single or multiple and usually round or ovoid, ranging in size from a few centimeters to patches covering large areas of the trunk . They are usually asymptomatic and lack inflammation. When lesions coalesce, they can form large, irregular, brown patches. The surface of the skin is normal in appearance, and there is no skin induration or sclerosis.
The borders or edges of these lesions are sharply defined, and they are usually described as abrupt, “cliff drop” borders ranging from 1 to 8 mm in depth, although they can have a gradual slant.31 These depressed patches are characteristic and give the impression of inverted plateaus, or, if multiple lesions are present, they can have the appearance of Swiss cheese. They are even more apparent when present on the back because the dermis is thicker in this area. The skin surrounding the patches is normal in appearance, and there is no erythema or lilac ring as in morphea.
COURSE
The course of this benign disease is progressive, and lesions can continue to appear for decades before reaching a standstill. Transformation to generalized morphea has not been observed.
HISTOPATHOLOGY
The histologic picture is generally not diagnostic. The epidermis is usually normal or slightly atrophic. Collagen bundles in the mid- and reticular dermis show varying degrees of homogenization and clumping. Dermal thickness is eventually reduced when compared with adjacent normal skin. Some irregular clumping and loss of elastic fibers were described in earlier case reports, but in most series, no abnormality was seen with elastic tissue stains; therefore, this is not of diagnostic value. The appendages are usually preserved. If sclerodermatous changes appear in pre-existing patches, the histology reveals varying degrees of collagen sclerosis resembling morphea.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis is to be made with active lesions of morphea that usually present as indurated, often hyperpigmented plaques with a characteristic peripheral lilac rim.
THERAPY
No treatment has been proved effective.