
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is a malignant neoplasm derived from nonkeratinizing cells that originate in the basal layer of the epidermis. If left untreated, BCC will continue to invade locally and may result in substantial tissue damage that compromises function and cosmesis. Metastasis is an extremely rare event.
EPIDEMIOLOGY
BCC is the most common cancer in humans. It is estimated that over 1 million new cases occur each year in the United States. BCC is more common in elderly individuals but is becoming increasingly frequent in people younger than 50 years of age. Christenson et al. noted a disproportionate increase in BCC in women under age 40. The malignancy accounts for approximately 75 percent of all non-melanoma skin cancers and almost 25 percent of all cancers diagnosed in the United States. The tumor characteristically develops on sun-exposed skin of lighter-skinned individuals, with 20 percent occurring on the nose. Men are affected slightly more often than are women. Levi et al. reported that the incidence of BCC rose steadily in the Swiss Canton of Vaud between 1976 and 1998 to levels of 75.1 in 100,000 in males and 66.1 in 100,000 in females.3,4 A study of non-melanoma skin cancers in Aruba supported these findings.5 In that study, BCC was the most common type of skin cancer diagnosed between 1980 and 1995. Tumors were more frequent in patients older than 60 years of age, and 57 percent were in men. The highest percentage of lesions occurred on the nose (20.9 percent), followed by other sites on the face (17.7 percent).
Risk factors for BCC have been well characterized and include ultraviolet light (UVL) exposure, light hair and eye color, northern European ancestry, and inability to tan.1 Patients with BCC are at increased risk for melanoma but not for other internal malignancies. Bower et al. reported that individuals with BCC had a threefold increased risk for melanoma but no increased risk for any other type of cancer.
ETIOLOGY AND PATHOGENESIS
The pathogenesis of BCC involves exposure to UVL, particularly the ultraviolet B spectrum (290 to 320 nm) that induces mutations in tumor suppressor genes. Some studies indicate that intermittent brief holiday exposures may place patients at higher risk than occupational exposure. Ramani and Bennett reported a significantly higher incidence of BCCs in World War II servicemen stationed in the Pacific theater than in those stationed in Europe. This suggests that several months or years of intense exposure to UVL may have deleterious long-term effects. Other factors that appear to be involved in the pathogenesis include mutations in regulatory genes, exposure to
ionizing radiation, and alterations in immunosurveillance.
BASAL CELL CARCINOMA AT A GLANCE
The propensity to develop multiple BCCs may be inherited. Included among heritable conditions predisposing to the development of this epithelial cancer are nevoid basal call carcinoma syndrome or basal cell nevus syndrome (BCNS), Bazex syndrome,15 and Rombo syndrome. Patients with BCNS may develop hundreds of BCCs and may exhibit a broad nasal root, borderline intelligence, jaw cysts, palmar pits, and multiple skeletal abnormalities. BCNS occurs due to mutations in the tumor suppressor PTCH gene
Bazex syndrome is transmitted in an X-linked dominant fashion.15 Patients have multiple BCCs, follicular atrophoderma, dilated follicular ostia with icepick scars, hypotrichosis, and hypohidrosis. In contrast, Rombo syndrome is transmitted in an autosomal dominant fashion. Patients have vermiculate atrophoderma, milia, hypertrichosis, trichoepitheliomas, BCCs, and peripheral vasodilation. Hypohidrosis is not a feature of Rombo syndrome .
The role of the immune system in the pathogenesis of skin cancer is not completely understood. Immunosuppressed patients with lymphoma or leukemia and patients who have received an organ transplant13 have a marked increase in the incidence of squamous cell carcinoma but only a slight increase in the incidence of BCC. Bastiaens et al. found that transplant recipients developed more BCCs on the trunk and arms than did nonimmunosuppressed patients.20 Patients with human immunodeficiency virus infection develop BCCs at the same rate as immunocompetent individuals, based on similar risk factors.21 Immunosuppressed long-term alcoholics tend to develop infiltrative BCCs with increased frequency.
A potential link between UVL and decreased immunity has been suggested by Gutierrez-Steil et al., who demonstrated that UVL-induced BCCs express Fas ligand (CD95L).23 They further showed that these cells were associated with CD95-bearing T cells undergoing apoptosis. This represents a potential mechanism by which UVL might help tumor cells avoid being killed by cytotoxic T lymphocytes.
▪ CLINICAL MANIFESTATIONS
Presentation
The presence of any friable, non-healing lesion should raise the suspicion of skin cancer. Frequently, BCC is diagnosed in patients who state that the lesion bled briefly then healed completely, only to recur. BCC usually develops on sun-exposed areas of the head and neck but can occur anywhere on the body. Features include translucency, ulceration, telangiectasias, and the presence of a rolled border. Characteristics may vary for different clinical sub-types, which include nodular, superficial, morpheaform, and pigmented BCCs and fibroepithelioma of Pinkus (FEP).
Basal Cell Carcinoma Sub-Types
NODULAR BASAL CELL CARCINOMA
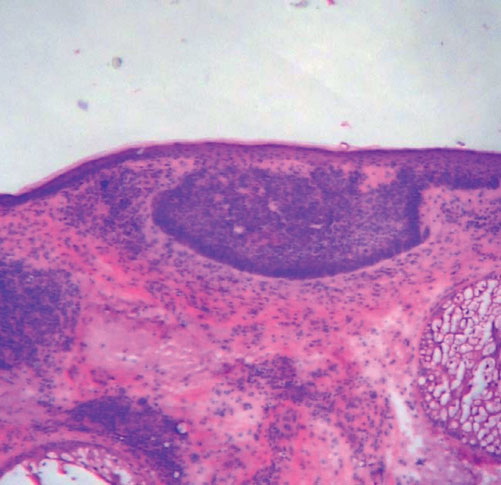
Nodular BCC is the most common clinical sub-type of BCC It occurs most commonly on the sun-exposed areas of the head and neck and appears as a translucent papule or nodule depending on duration. There are usually telangiectasias and often a rolled border. Larger lesions with central necrosis are referred to by the historical term rodent ulcer (Fig. 115-2). The differential diagnosis of nodular BCC includes traumatized dermal nevus and amelanotic melanoma.
PIGMENTED BASAL CELL CARCINOMA
Pigmented BCC is a sub-type of nodular BCC that exhibits increased melanization. Pigmented BCC appears as a hyperpigmented, translucent papule, which may also be eroded (Fig. 115-3). The differential diagnosis includes nodular melanoma.
SUPERFICIAL BASAL CELL CARCINOMA
Superficial BCC occurs most commonly on the trunk and appears as an erythematous patch (often well demarcated) that resembles eczema An isolated patch of “eczema” that does not respond to treatment should raise suspicion for superficial BCC.
MORPHEAFORM (SCLEROSING) BASAL CELL CARCINOMA
Morpheaform BCC is an aggressive growth variant of BCC with a distinct clinical and histologic appearance. Lesions of morpheaform BCC may have an ivory-white appearance and may resemble a scar or a small lesion
of morphea . Thus, the appearance of scar tissue in the absence of trauma or previous surgical procedure or the appearance of atypical-appearing scar tissue at the site of a previously treated skin lesion should alert the clinician to the possibility of morpheaform BCC and the need for biopsy.
FIBROEPITHELIOMA OF PINKUS
FEP classically presents as a pink papule, usually on the lower back. It may be difficult to distinguish from an acrochordon or skin tag.
▪ BIOLOGIC BEHAVIOR
Local Invasion
The greatest danger of BCC results from local invasion . In general, BCC is a slow-growing tumor that invades locally rather than metastasizes. The doubling time is estimated to be between 6 months and 1 year. If left untreated, the tumor will progress to invade subcutaneous tissue, muscle, and even bone. Anatomic fusion planes appear to provide a lowresistance path for tumor progression. Tumors along the nasofacial or retroauricular sulcus may be extensive. In one informative case, a patient documented the progression of his own tumor with photographs over a 27-year period. The lesion, which encompassed an entire side of the face, including the maxillary sinus, apparently doubled over a 10-year period and grew rapidly in the 2 years before hospital admission. This scenario occurs in the context of physical or psychiatric disability that interferes with judgment or access to health care. In another case, a 35-cm BCC on the back of a 65-year-old man recurred after wide local excision and x-ray therapy (XRT), resulting in spinal cord compression. Lethal extension to the central nervous system from aggressive scalp BCC has been reported.
Perineural Invasion
Perineural invasion is uncommon in BCC and occurs most often in histologically aggressive or recurrent lesions. In one series, Niazi and Lamberty identified perineural invasion in fewer than 0.2 percent of cases.31 In that series, perineural BCC was seen most often with recurrent tumors located in the preauricular and malar areas. Ratner et al. found a higher incidence in their study (3.8 percent). Leibovitch et al. reported perineural spread in more than 50 percent of periocular BCCs eventuating in orbital invasion. These tumors required extensive surgery and in some cases exenteration Perineural spread may manifest as pain, paresthesias, weakness, or paralysis. The presence of focal neurologic symptoms at the site of a previously treated skin cancer should raise concern about nerve involvement.
Metastasis
Metastasis of BCC occurs only rarely, with rates varying from 0.0028 percent to 0.55 percent.34-36 Involvement of lymph nodes and lungs is most common. Von Domarus et al. reported five cases of metastatic BCC in which perineural or intravascular invasion had been noted in three.37 Squamous differentiation was not observed in the primary tumors in the cases they presented but was noted in two of five cases of metastatic cancer. Overall, squamous differentiation was present in 15 percent of the primary or metastatic tumors from the 170 cases reviewed. Aggressive histologic characteristics, including morpheaform features, squamous metaplasia, and perineural invasion, have been identified as risk factors for metastasis.36
DIAGNOSIS
Diagnosis of BCC is accomplished by accurate interpretation of the skin biopsy results. The preferred biopsy methods are shave biopsy, which is often sufficient, and punch biopsy. A sterilized razor blade, which can be precisely manipulated by the operator to adjust the depth of the biopsy specimen, is often superior to a No. 15 scalpel for shave biopsies. A punch biopsy may be useful for flat lesions of morpheaform BCC or for recurrent BCC occurring in a scar.
HISTOPATHOLOGY
Histopathologic features vary somewhat with sub-type, but most BCCs share some common histologic characteristics.
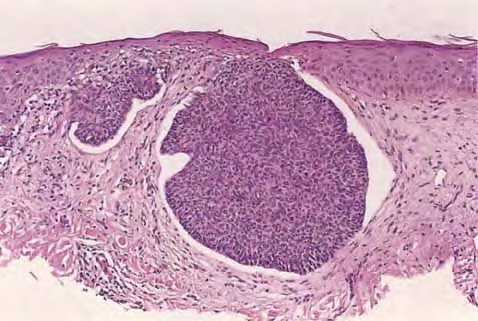
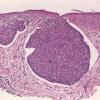
The malignant basal cells have large nuclei and relatively little cytoplasm. Although the nuclei are large, they may not appear atypical. Usually, mitotic figures are absent. Frequently, retraction of stroma from tumor islands is present, creating peritumoral lacunae that are helpful in histopathologic diagnosis.
Nodular Basal Cell Carcinoma
Nodular BCCs account for half of all BCCs and are characterized by nodules of large basophilic cells and stromal retraction . The term micronodular BCC is used to describe tumors with multiple microscopic nodules smaller than 15µm .
Pigmented Basal Cell Carcinoma
Pigmented BCC shows histologic features similar to those of nodular BCC but with the addition of melanin.38 Approximately 75 percent of BCCs contain melanocytes, but only 25 percent contain large amounts of melanin. The melanocytes are interspersed between tumor cells and contain numerous melanin granules in their cytoplasm and dendrites. Although the tumor cells contain little melanin, numerous melanophages populate the stroma surrounding the tumor.
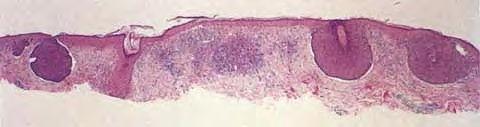
Superficial Basal Cell Carcinoma
Superficial BCC is characterized microscopically by buds of malignant cells extending into the dermis from the basal layer of the epidermis. The peripheral cell layer shows palisading. There may be epidermal atrophy, and dermal invasion is usually minimal. This histologic sub-type is encountered most often on the trunk and extremities but may also appear on the head and neck. There may be a chronic inflammatory infiltrate in the upper dermis.
Morpheaform Basal Cell Carcinoma
Morpheaform or infiltrative BCC consists of strands of tumor cells embedded within a dense fibrous stroma . Tumor cells are closely packed and, in some cases, only one cell thick. Strands of tumor extend deeply into the dermis. The cancer is often larger than the clinical appearance indicates. Recurrent BCC may also demonstrate infiltrating bands and nests of cancer cells embedded within the fibrous stroma of scar.
Fibroepithelioma of Pinkus
In FEP, long strands of interwoven basiloma cells are embedded in fibrous stroma.38 Histologically, FEP shows features of reticulated seborrheic keratoses and superficial BCC.
TREATMENT
Management of BCC is guided by anatomic location and histologic features. Approaches include Mohs micrographic surgery (MMS), standard surgical excision, destruction by various modalities, and topical chemotherapy. The best
chance to achieve cure is through adequate treatment of primary BCC, because recurrent tumors are more likely to recur and to cause further local destruction.
Differential Diagnosis of Basal Cell Carcinoma (BCC)
- o Dermal nevus
- o Squamous cell carcinoma
- o Appendageal tumor
- o Dermatofibroma
- o Scar
- o Seborrheic keratosis
- o Nodular melanoma
- o Superficial spreading melanoma
- o Lentigo maligna melanoma
- o Appendageal tumor
- o Compound nevus
- o Blue nevus
- o Bowen disease
- o Mammary or extramammary Paget disease
- o Superficial spreading melanoma
- o Single plaque of psoriasis
- o Single plaque of eczema
- o Scar
- o Morphea
- o Trichoepithelioma
- · Fibroepithelioma of Pinkus
- o Skin tag
- o Papillomatous dermal nevus
- o Fibroma
Mohs Micrographic Surgery
MMS offers superior histologic analysis of tumor margins while permitting maximal conservation of tissue compared with standard excisional surgery. Rowe, Carroll, and Day report a recurrence rate of 1 percent for primary BCCs treated by MMS.40 This was superior to the rate for other modalities, including standard excision (10 percent), curettage and desiccation (C&D) (7.7 percent), XRT (8.7 percent), and cryotherapy (7.5 percent). Recurrent BCCs treated by MMS reappeared at a rate of 5.6 percent, which was again superior to the rate for other modalities, including excision (17.6 percent), XRT (9.8 percent), and C&D (40 percent). MMS is the treatment of choice for morpheaform, poorly delineated, incompletely removed, and otherwise high-risk primary BCCs. It is the preferred treatment for recurrent BCC and for any BCC that occurs at a site where tissue conservation is desired. MMS is particularly useful in treating BBCs at high-risk anatomic sites, including the embryonic fusion planes represented by the nasofacial junction and retroauricular sulcus .
Standard Excision
Compared with non-excisional techniques, standard surgical excision offers the advantage of histologic evaluation of the removed specimen. Although standard excision is appropriate for many BCCs, cure rates for standard excisional surgery are inferior to those for MMS in cases of primary morpheaform BCCs, recurrent BCCs, and tumors located in high-risk anatomic sites. Wolf and Zitelli demonstrated that margins of 4 mm were adequate for 95 percent of nonmorpheaform BCCs smaller than 2 cm in diameter when treated by standard excision. Johnson, Tromovitch, and Swanson reported a 96.7 percent cure rate when the excision included a 2-mm margin beyond the area defined by curettage. Tumor was present in 64 of 403 curette margins and in 12 of 403 excision
margins. The histologic sub-type was aggressive in 11 of 12 cases with positive excision margins. Margins of 5 mm are necessary for primary morpheaform BCC or recurrent BCC. Excision of primary BCC should extend to fat to ensure adequate tumor removal.
|
Indications for Mohs Surgery for Basal Cell Carcinoma
|
- · Location on a high-risk anatomic site including mask area of face, scalp, anatomic fusion planes, periorbital area/eyelid
- · Tumor > 2 cm
- · Aggressive histologic sub-type
- · Recurrent tumor
- · Incompletely excised basal cell carcinoma
- · Location on previously irradiated skin
- · Immunosuppression of patient after solid organ transplantation
- · Indistinct clinical border
- · Situation requiring conservation of normal tissue to preserve function and cosmesis
- · Situation requiring highest achievable probability of cure to preserve function and cosmesis
|
|
Curettage and Desiccation
C&D is one of the most frequently used treatment modalities for BCC. That C&D is operator dependent was shown by Kopf et al., who identified a significant difference in cure rate between patients treated by private practitioners (94.3 percent) and those treated by residents (81.2 percent). Spiller and Spiller reported a cure rate of 97 percent in 233 patients.46 Cure rate decreased as a function of primary lesion size: for lesions smaller than 1.0 cm, the cure rate was 98.8 percent; for lesions between 1.0 and 2.0 cm, 95.5 percent; and for lesions larger than 2.0 cm, 84 percent. Recurrences were noted most often on the forehead, temple, ears, nose, and shoulders. C&D is not recommended for large primary BCC, morpheaform BCC, or recurrent BCC.
Cryosurgery
Cryosurgery is another destructive modality that has been used in the treatment of BCC.47 Two freeze-thaw cycles with a tissue temperature of -50°C (-58°F) are required to destroy BCC. In addition, a margin of clinically normal tissue must be destroyed to eradicate sub-clinical extension. Cryosurgery lacks the benefit of histologic confirmation of tumor removal. Kuflik and Gage reported 99 percent cure rates in 628 patients followed for 5 years.48 Possible complications of cryosurgery include hypertrophic scarring and post-inflammatory pigmentary changes. Another serious potential adverse outcome is the obscuring of tumor recurrence by fibrous scar tissue. Any recent change in a cryosurgery scar after normal healing is completed should raise the suspicion of recurrent BCC.
Topical Treatment
IMIQUIMOD
Imiquimod (5 percent cream) has been used in the treatment of skin cancers.49 Imiquimod is a Toll-like receptor 7 agonist and is believed to induce interferon-α and other cytokines to boost T helper 1 type immunity. In two double-blind, randomized, vehicle-controlled trials, clinical and histologic clearance rates for dosing five and seven times per week were 75 percent and 73 percent, respectively, for superficial BCC.50,51 In another study, 10 of 19 nodular BCCs (approximately 53 percent) cleared after treatment with imiquimod.52 In general, adverse side effects are limited to local skin reactions. Follow-up in case series has generally been shorter than that in retrospective studies of recurrence rates after definitive surgical management.
5-FLUOROURACIL
5-Fluorouracil (5-FU), a topically applied chemotherapeutic agent used in the treatment of actinic keratoses, has also been used to treat BCCs. In one series, Epstein showed a 5-year recurrence rate of 21 percent after 5-FU treatment, which was reduced to 6 percent when curettage was performed initially. 5-FU is metabolized by dihydropyrimidine dehydrogenase, and its use is contraindicated in patients deficient in that enzyme. The use of 5-FU to treat BCC should be considered carefully and should include an evaluation of the risk of recurrence and treatment failure.
Photodynamic Therapy
Photodynamic therapy involves the activation of a photosensitizing drug by visible light to produce activated oxygen species that destroy the constituent cancer cells.56 Exogenous δ-aminolevulinic acid increases intracellular production of the endogenous photosensitizer protoporphyrin type IX, which preferentially accumulates in tumor cells. Morrison et al.59 reported an 88 percent initial clearance of 40 large (> 2 cm) BCCs after one to three treatments. The time of follow-up was between 12 and 60 months. Reports of higher recurrence rates by others suggest that this method may be best reserved for select situations in which better established methods are not feasible.57 Marmur et al. reviewed photodynamic therapy for non-melanoma skin cancer and reported recurrence rates ranging from 0 percent to 31 percent for BCC.57
Radiation Therapy
XRT may be useful in cases of primary BCC or in cases in which postsurgical margins are positive for cancer. Advantages include minimal patient discomfort and avoidance of an invasive procedure for a patient unwilling or unable to undergo surgery. Potential disadvantages include lack of histologic verification of tumor removal, prolonged treatment course, cosmetic result that may worsen over time, and predisposition to aggressive and extensive recurrences. Local control rates of 93 percent to 97 percent have been reported; however, cosmesis has been rated inferior to results achieved surgically.
Special Management Issues
INCOMPLETELY EXCISED BASAL CELL CARCINOMA
Based on data from the 1960s suggesting that 50 percent to 70 percent of incompletely excised BCCs do not recur, some physicians adopted a “wait and see” approach. In some cases, flap and graft repair may have been performed before confirmation of negative margins, so that the anatomy was distorted. This confounds identification of positive margins for definitive treatment. Incomplete resection was addressed by Robinson and Fisher, who reported on 994 patients consecutively referred for treatment of incompletely excised BCCs with subsequent clinical recurrence. Of these, only 32 were referred for MMS for complete tumor removal at the time the original operating surgeon received the pathologic confirmation of positive excision margins. For the remaining 962 recurrent BCCs, the nose was the most common anatomic site (43 percent), and flap repair was the most common form of reconstruction (52 percent). The authors recommend MMS for the treatment of incompletely excised BCC. Ideally, patients should receive treatment at the time of diagnosis, because delay will likely result in increased local tissue damage . Patients unable to undergo re-excision to achieve clear margins should be evaluated for XRT.
NEUROTROPIC BASAL CELL CARCINOMA
Perineural invasion by BCC is a rare event (< 0.2 percent of cases).32,33 When perineural invasion is detected, every effort should be made to clear the tumor, preferably by MMS. Patients with gross perineural invasion manifested by neurologic symptoms would benefit from preoperative magnetic resonance imaging to assess extent of tumor spread. Classic examples include brow paralysis due to involvement of the temporal branch of the facial nerve and mid-face paresthesias secondary to involvement of the trigeminal nerve.
METASTATIC BASAL CELL CARCINOMA
Although it is exceedingly rare, the possibility of metastatic disease exists and may need to be addressed.36 If nodal disease is suspected on surgical examination, lymph node biopsy and imaging studies, as well as evaluation by medical and surgical oncologists, are indicated. Platinum-based chemotherapy has been used with modest results in treatment of metastatic BCC; however, rapid clinical response was reported using a combination of cisplatin and paclitaxel.62
▪ COURSE AND PROGNOSIS
With appropriate treatment, the prognosis for most patients with BCC is excellent. Control rates as high as 99 percent have been achieved by MMS. Although tumor control rates for primary tumors are high, patients must be monitored for recurrence and development of new primary BCCs. The risk for development of a second primary BCC ranges from 36 percent to 50 percent.63 Periodic full-body skin examinations and counseling about sun protection are recommended for any patient with a history of BCC. This is especially important because patients with a history of BCC are at increased risk for melanoma.
The prognosis for patients with recurrent BCC is favorable, although recurrent tumors are more likely to appear again and to behave aggressively. Patients with a history of recurrent disease must be monitored more frequently for the development of further recurrences and new primary tumors. For the rare patient with metastatic disease, prognosis is poor, with a mean survival of 8 to 10 months from the time of diagnosis.