|
Superficial Spreading Melanoma
Superficial spreading melanoma, also referred to as pagetoid melanoma , is the most frequent form of melanoma (about 70% of all cases), and may therefore be regarded as the "common" or "prototypic" form of melanoma. These lesions were described in the past as "atypical melanocytic hyperplasia" or "precancerous melanosis," a term that dates to one of the earliest descriptions of melanoma by Dubreuilh in 1912 . The lesions, which occur in a relatively young to middle-aged patient population, may occur on exposed skin but are more commonly found on intermittently exposed skin and are rare on unexposed skin. In contrast to lentigo maligna, superficial spreading melanoma is believed to be associated with acute intermittent rather than chronic continuous sun exposure, which is often recreational rather than occupational . The most frequently involved sites are the upper back, especially in men, and the lower legs, especially in women. The lesions are slightly or definitely elevated, with a palpable border and an irregular outline. There is often variation in color that includes not only tan, brown, and black, but also pink, blue, and gray. White areas may be seen at sites of spontaneous regression . Microinvasion may be clinically unapparent, but the onset of tumorigenic vertical growth is indicated by the development of a papule followed by nodularity and sometimes also ulceration, the latter usually a late feature. In rare instances the lesion has a verrucous surface, in which case differentiation from a seborrheic keratosis may be difficult . In its early stage of development, superficial spreading melanoma may be indistinguishable clinically from a dysplastic nevus. Although dermoscopy can improve clinical diagnostic specificity , histologic examination remains the gold standard and is necessary for accurate diagnosis .
|
|
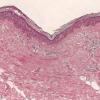
Histopathology.
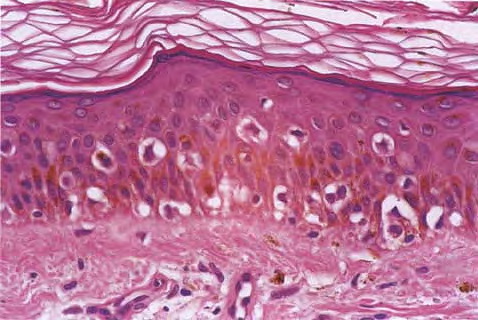
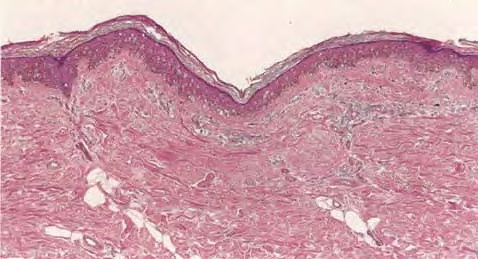
Architectural pattern features of importance in the diagnosis include the large diameter of the lesions, poor circumscription (the last cells at the edge of the lesion tending to be small, single, and scattered), and asymmetry (one half of the lesion does not mirror the other half) . The epidermis is irregularly thickened and thinned, in contrast to the uniformly elongated rete ridge pattern of a dysplastic nevus . Rather uniformly rounded, large melanocytes are scattered in a pagetoid pattern throughout the epidermis. The large cells lie predominantly in nests in the lower epidermis and singly in the upper epidermis. The nests tend to vary a good deal in size and shape and to become confluent. Dermal melanophages and a dermal infiltrate are regularly present. The lymphocytic infiltrate may be patchy and perivascular as in a dysplastic nevus but is typically dense and bandlike, especially in invasive lesions.
|
|
Cytologically, the lesional cells are rather uniform and have abundant cytoplasm containing varying amounts of melanin that often consists of small, "dusty" granules. They are almost entirely devoid of readily visible dendrites. The nuclei tend to be large and hyperchromatic, with irregular nuclear membranes and irregularly clumped chromatin . This uniform cytologic atypia is of considerable diagnostic importance and contrasts with the random cytologic atypia of dysplastic nevi.
When the lesion is in situ, the basement membrane is intact and there are no lesional cells in the dermis. In an invasive but nontumorigenic lesion (invasive radial growth phase or microinvasive melanoma), cells similar to those in the epidermis are present in the dermis in the form of small nests, with no nests larger than those in the epidermis, and with no dermal mitoses . When tumorigenic vertical growth phase is present, there is at least one, or often more than one, cluster of cells in the dermis that is larger than the largest intraepidermal nest, and/or there may be lesional cell mitoses in the dermis .
|
|
Histogenesis. On electron microscopic examination, melano-somes are present in great numbers in the large pagetoid tumor cells. Their shape is largely spheroid, rather than ellipsoid as in normal melanocytes and in the tumor cells of lentigo maligna . They often also show other abnormalities, such as absence of cross-linkages of the filaments within the melanosomes. Melanization within the melanosomes is variable but often incomplete . This accounts for the finely divided "dusty" character of the pigment in the cells of many melanomas. As already mentioned, it is likely that most superficial spreading melanomas have mutually exclusive activating mutations of the oncogene BRAF or NRAS. In a recent genotype-phenotype study, melanomas that had prominent nesting and pagetoid scatter of melanocytes-criteria similar to those for superficial spreading melanoma-were
|
|
more likely than other melanomas to be associated with BRAF or NRAS mutations . These evolving genetic data will lead to refinement of the clinicopathologic melanoma classification system in the near future.
|
|
Differential Diagnosis. A junctional nevus differs from superficial spreading melanoma in radial growth phase by a lack of atypia in the tumor cells, particularly in their nuclei, by a lack of pagetoid upward extension of tumor cells, by the absence of a significant inflammatory infiltrate in the upper dermis, and often but not always by a sharper lateral demarcation. Salient features in the important distinction from junctional melanocytic dysplasia have been reviewed , and include, at scanning magnification, larger size, asymmetry, an irregularly thickened and thinned epidermis, and a bandlike lymphocytic infiltrate in superficial spreading melanoma. At higher power, indicators of melanoma include the presence of high-level and extensive pagetoid melanocytosis (large neoplastic cells scattered among benign keratinocytes), high-grade and/or uniform cytologic atypia, and lesional cell mitoses (the latter present in about one third of cases). A junctional Spitz nevus, especially the uncommon pagetoid Spitz nevus, may simulate superficial spreading melanoma quite closely. Distinguishing features include generally smaller size, the presence of large spindle and/or epithelioid cells, the presence of Kamino bodies, and the lack of "consumption" or thinning of the epidermis above the lesion, as previously discussed (see section Spitz Nevus). The so-called nevi of special sites, including flexural sites, ears, scalp, and breast, may also simulate this form of melanoma in particular, and these should be seriously considered when a biopsy from one of these sites is examined . Caution should be exercised when what at first appears as melanoma in situ is restricted to the epidermis that overlies a surgical or traumatic scar because this must be differentiated from the recurrent nevus phenomenon [see section Recurrent Nevus (Pseudomelanoma)]. Helpful features include the precise spatial restriction of the atypical intraepidermal focus to the zone overlying (but not extending horizontally beyond) the scar, the presence of residual nevus cells, and the absence of true uniform cytologic atypia. Whenever possible, it is important to also review the initial biopsy in such cases. The differential diagnostic distinction from lentiginous melanomas is of less consequence because the management is the same. In lentigo maligna, the epidermis is atrophic and pagetoid melanocytosis is less prominent, and contiguous replacement of the basal cell layer by atypical melanocytes is the dominant pattern. Problematic cases can be reported as malignant melanoma (in situ or microinvasive, etc.) without designation as to type.
|
|
When tumorigenic vertical growth phase is present, it does not differ appreciably from that in any other form of melanoma, except for the adjacent radial growth phase . Classification of such complex tumorigenic primary melanomas is based on the morphology of the radial growth phase.
|
|
Among the nonmelanocytic neoplasms that must be differentiated from a superficial spreading melanoma in situ are Paget's disease and pagetoid examples of Bowen's disease (squamous cell carcinoma in situ). Paget's disease usually shows remnants of compressed basal cells beneath the tumor cells, whereas in superficial spreading melanoma the lesional cells extend to the basement membrane. In Paget's disease, the tumor cells may stain positively for carcinoembryonic
|
|
antigen and keratin and are negative for HMB-45 and Melan-A. S100 reactivity, although unusual, may occasionally be observed in Paget's disease. Pagetoid Bowen's disease (discussed in Chapter 29) shows, as a rule, a wellpreserved basal cell layer, except in areas in which dermal invasion has taken place, and immunohistochemically the atypical cells stain positively with antikeratin antibodies (e.g., AE1/AE3) . They do not stain with S100 or with Melan-A or HMB-45. It should be noted that the cells of Paget's disease and of Bowen's disease may contain melanin pigment because of transfer from reactive melanocytes in the adjacent skin.
|
|
A final pitfall in evaluating nonmelanocytic mimics of intraepidermal melanoma involves the variable tendency of keratinocytes within the uppermost epidermal layers to exhibit perinuclear retraction presumably due to cytoplasmic glycogenation combined with tissue processing. Some body sites (e.g., areola and along the milk line) may be particularly prone to this change, perhaps in part the result of so-called "clear cells of Toker." These cells may produce the false appearance of true pagetoid spread in an otherwise benign or dysplastic melanocytic lesion, thus inciting consideration of a diagnosis of superficial spreading melanoma. However, keratinocytes so altered are recognizable at high magnification as cells with nuclei surrounded by clear spaces (retraction clefts) that themselves are bordered by a rim of cytoplasm and joined by desmosomes, in contrast to pagetoid melanoma cells, which lack desmosomes and whose nuclei are directly enveloped by relatively clear cytoplasm that may be surrounded by a thin, clear mantle of retraction that separates the cell from adjacent keratinocytes.
|
|