|
Subcorneal Pustular Dermatosis = الجلاد البثري تحت الطبقة المتقرنة |
 |
 |
 |
|
Sub corneal Pustular Dermatosis
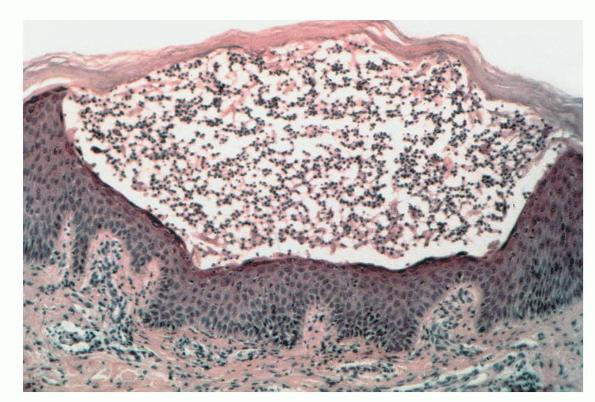
SPD (Sneddon-Wilkinson disease) is a chronic disorder that was first described in 1956 and is characterized by superficial sterile pustules that have a predilection for flexural surfaces and the axillary and inguinal folds. Many cases have been shown to be a variant of IgA pemphigus . It usually spares the face and mucous membranes. The pustules develop in an annular or polycyclic arrangement. Pus characteristically accumulates in the lower half of large pustules.
|
|
SPD may be associated with a monoclonal gammopathy, which most commonly is an IgA paraproteinemia. Some of these cases eventuate in an IgA myeloma and may have IgA squamous intercellular substance deposits.
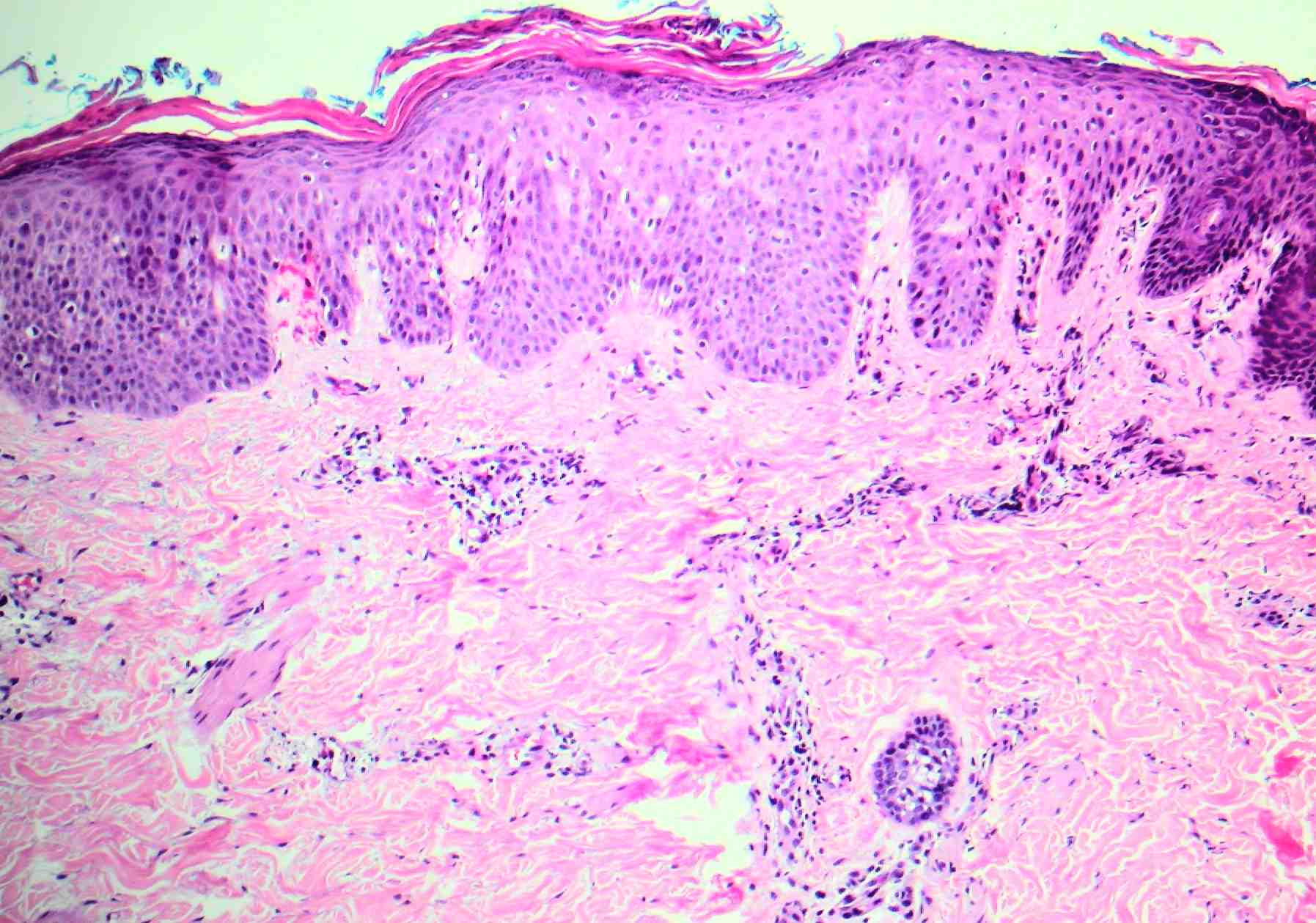
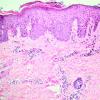
Histopathology.
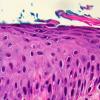
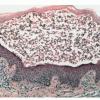
The pustules are subcorneal and contain neutrophils, with only an occasional eosinophil .
|
|
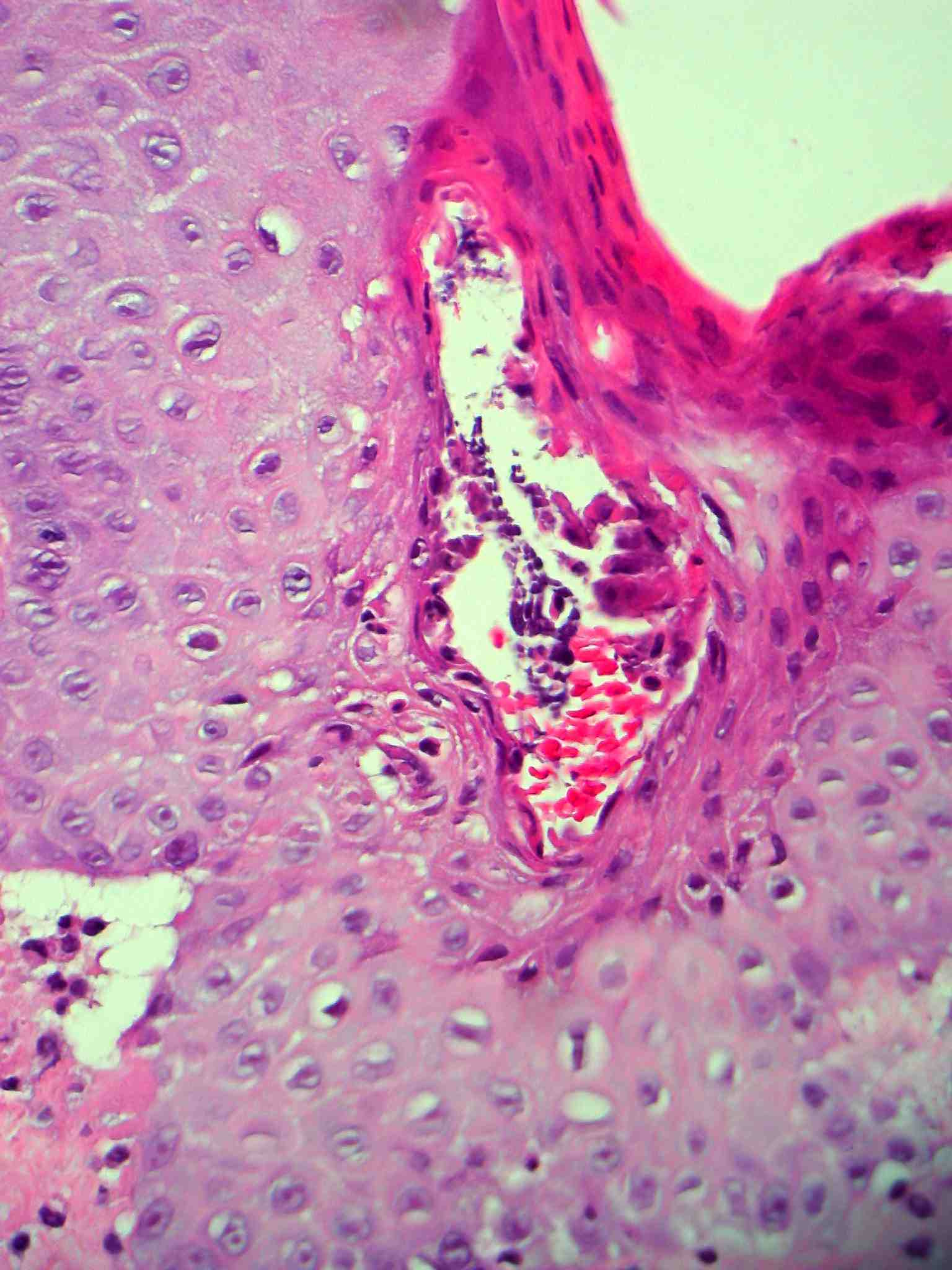
The underlying slightly edematous stratum malpighii contains a small number of neutrophils. Only a few spongiform pustules are formed. In some instances, a few acantholytic cells are found in the base of the pustule, most likely because of proteolytic enzymes present in the pustular contents. They may be partially attached to the epidermis or may lie free in the pustule among the neutrophils. The dermal papillae contain dilated capillaries and a perivascular infiltrate composed of neutrophils and a few eosinophils and mononuclear cells.
|
|
Pathogenesis. The squamous intercellular substance IgA leads to neutrophilic infiltration. In some patients, elevated levels of tumor necrosis factor-a in the serum and pustules may be responsible for neutrophil activation (137).
|
|
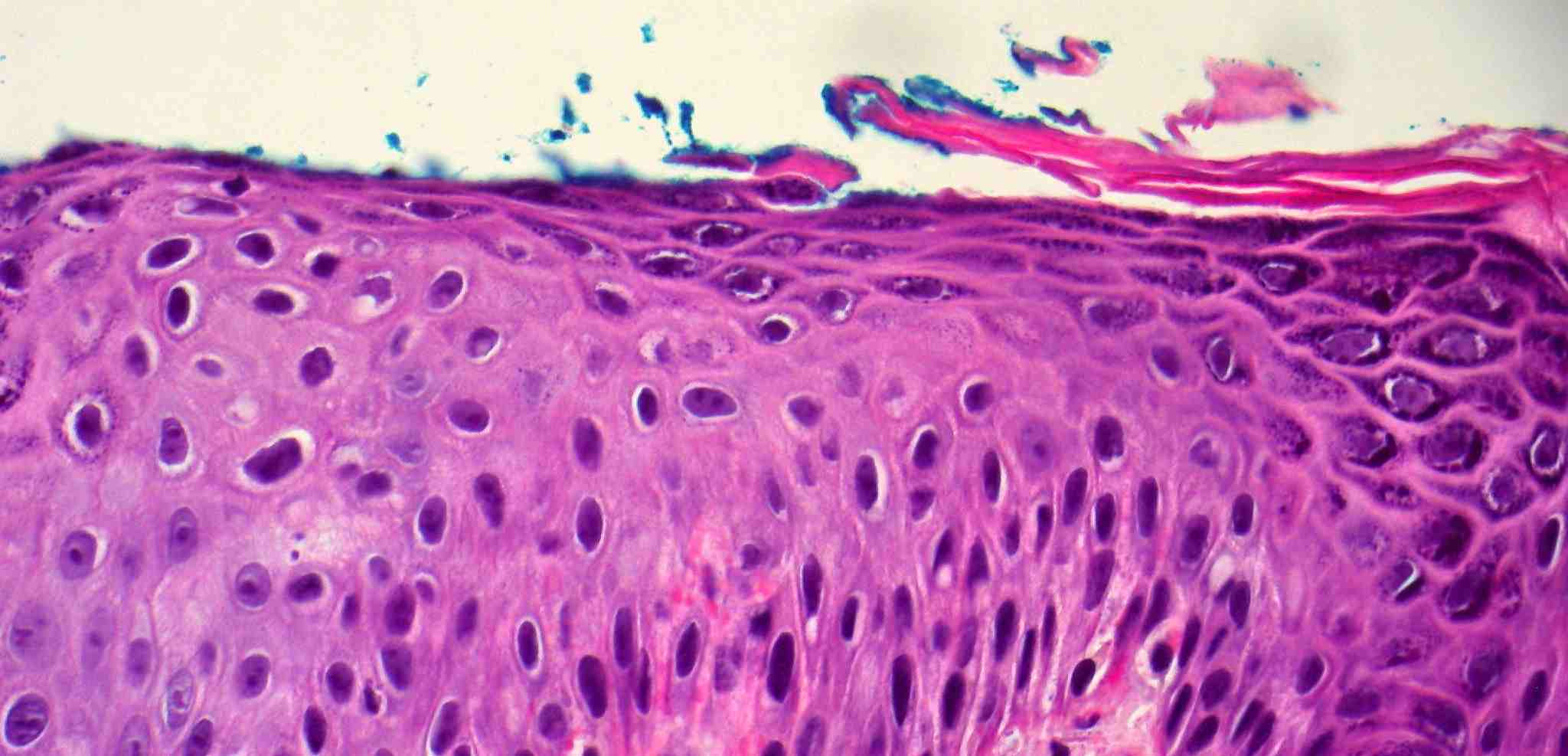
Ultrastructural Study. The edge of the pustules shows cytolytic changes in the upper epidermis, especially in the granular layer. Dissolution of the plasma membrane and of the cytoplasm of granular cells causes the formation of a subcorneal split. The transepidermal migration of neutrophils and their subcorneal accumulation are regarded as events secondary to the cellular destruction in the stratum granulosum seen in one study.
|
|
Differential Diagnosis. The differential diagnosis includes other entities that show subcorneal pustules. Histologic differentiation from impetigo may be impossible unless bacteria can be demonstrated with a Gram stain. Cultures may be necessary for diagnosis. Histologic differentiation from pemphigus foliaceus or pemphigus erythematosus may also be difficult, as both diseases show subcorneal blisters with acantholysis, although the acantholysis tends to be more pronounced in pemphigus than in SPD. Clinical information, IF testing, and a therapeutic trial of sulfones may be necessary for definitive diagnosis.
|
|
Although subcorneal pustules occur in both pustular psoriasis and SPD, spongiform pustules occur only in pustular psoriasis. Some authors regard SPD as a variant of pustular psoriasis, but with the association to IgA gammopathies and squamous intercellular substance deposits of IgA, this view is discredited.
|
|