PIGMENTED
SPINDLE CELL
NEVUS
Epidemiology
The mean age of presentation has been reported as 25.3 years, ranging from 2.5 to 56.0 years of age. Similar age ranges have been reported in other studies. The majority of cases occur in the third decade of life. Female patients outnumber male patients with reported ratios of 2:1, 1.4:1.0, and 1.3:1.0. The majority of these lesions are found on the extremities with reported frequencies of 67.0 percent, 69.6 percent, and 75.0 percent. There is a preference for the lower extremity, especially the thigh, with the back being the next most common site.
Etiology and Pathogenesis
It may be presumed that PSCN are derived from the same progenitor cells giving rise to epidermal melanocytes and nevomelanocytes. No known specific mutation has been identified.
PIGMENTED SPINDLE CELL NEVUS AT A GLANCE
· Acquired, benign melanocytic tumors comprised of heavily pigmented spindle-shaped melanocytic cells confined primarily to the epidermis.
· The pigmented spindle cell presents as a jet black lesion often with “starburst” appearance.
· These nevi are thought to develop quickly and then stabilize.
· Malignant degeneration is thought to be rare.
· Synonyms: Reed nevus, pigmented Spitz nevus.
HISTORY
PSCN was first described by Reed in 1975.These lesions are generally detected as acquired lesions, often during the third decade of life. At presentation, patients often note that the lesion has increased in size. It is not known how quickly these lesions grow, but growth may be relatively rapid as one case report of a lesion on a 3-year-old child documented significant growth over a 3- and 6-month period. Once fully developed, it is assumed that these lesions will remain stable, but the full natural history of these lesions is not well characterized.
CUTANEOUS LESIONS
The PSCN is usually a sharply circumscribed, uniformly darkly pigmented papule. Dermoscopically, most of the lesions are jet black but may be blue-gray or brown. In the initial growth phase, the lesions may have a globular appearance but the vast majority of these lesions are uniformly dark centrally, with a sharp interface with surrounding skin often exhibiting streaks/pseudopods and giving the lesion a starburst appearance.
RELATED PHYSICAL FINDINGS
No known association.
Laboratory Tests
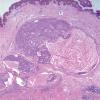
HISTOPATHOLOGY
PSCN consists of vertically oriented fascicles of spindle-shaped, pigment-producing melanocytes ; some pagetoid upward migration may be present, but the lesion can be distinguished from melanoma by uniform nuclei, uniform cellular detail, and distinctive pattern of growth. Almost all cases of pigmented spindle cell nevus have a lymphohistiocytic host response. Spindle cells extend down eccrine ducts in 40 percent and involve hair follicles in 22 percent of lesions. There is an overlap of these lesions with Spitz nevi. In a review of 91 PSCN by Sagebiel et al., cells were predominantly spindle in 74 percent and mixed spindle cell and epithelioid cell in 26 percent of patients. There are atypical variants of PSCN in which there are architectural alterations and striking cellular atypia.
SPECIAL TESTS
No known specific mutation or genetic markers.
Complications
There are no reported complications, but misinterpretation of benign or malignant behavior of the lesion could result in unnecessary or insufficient treatment, respectively.
Prognosis and Clinical Course
The PSCN are thought to be benign. No local recurrence or distant spread was noted for 38 patients followed for an average of 14 months. In another study, 57 patients were followed for an average of 6 years and again no local recurrence or metastasis was noted.
Treatment
If there is clinical concern, these lesions should be excised with a narrow margin of normal skin.
Differential Diagnosis of Pigmented Spindle Cell Nevus
· Spitz nevus
· Blue nevi
· Hematoma
· Atypical nevomelanocyte
· Melanoma
Prevention
The role of UVR exposure in the development of PSCN is unknown. Generally, it is best to avoid UVR overexposure.

