|
SeBborrheic dermatitis = التهاب الجلد الدهني |
 |
 |
 |
|
Seborrheic Dermatitis
Clinically, patients develop erythema and greasy scale on the scalp, ears, eyebrows, nasolabial areas, and central chest. Rarely, patients with seborrheic dermatitis develop generalized lesions. In infants, the scalp ("cradle cap"), face, and diaper areas are often involved. It is said to be a rare cause of erythroderma. Seborrheic dermatitis is seen with increased frequency in patients with Parkinson's disease, epilepsy, congestive heart failure, chronic alcoholism, zinc deficiency, and HIV infection. Patients with HIV infection often have severe refractory disease and atypical distribution .
|
|
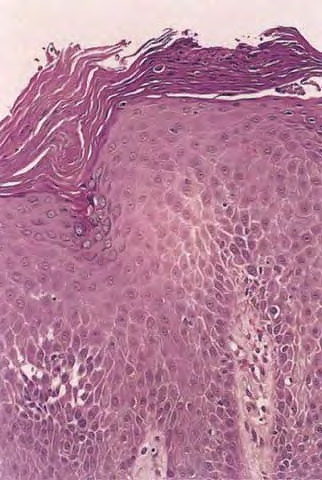
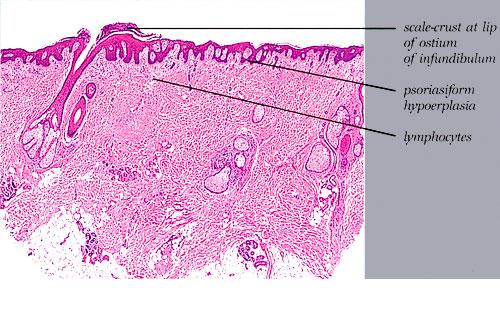
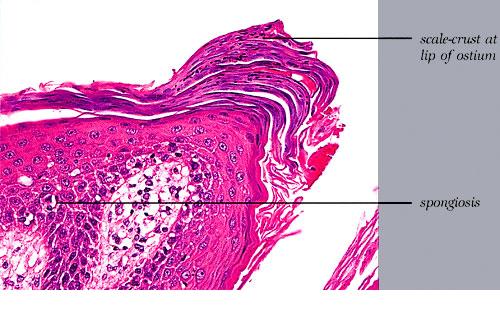
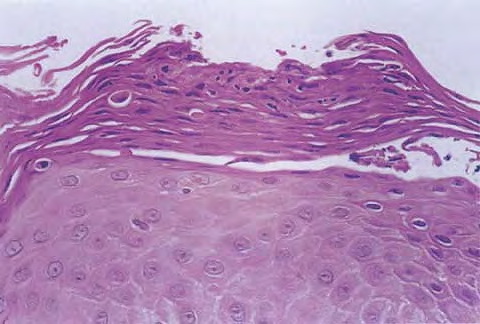
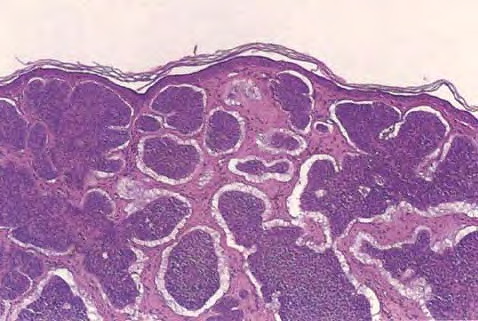
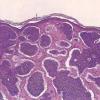
Histopathology.
The histopathologic features are a combination of those observed in psoriasis and spongiotic dermatitis. Mild cases may exhibit only slight subacute spongiotic dermatitis. The stratum corneum contains focal parakeratosis, with a predilection for the follicular ostia, a finding known as shoulder parakeratosis . Occasional pyknotic neutrophils are present within parakeratotic foci {neutrophilic parakeratosis}, sometimes with fluid {neutrophilic crust}. There is moderate acanthosis with regular elongation of the rete ridges, mild spongiosis, and focal exocytosis of lymphocytes. The dermis contains a sparse mononuclear cell infiltrate. In HIV-infected patients, the epidermis contains apoptotic keratinocytes, and the dermal infiltrate usually contains plasma cells.
|
|
Pathogenesis. The pathogenesis is unknown; the role of Malassezia sp. {Pityrosporum} in the etiology is controversial even though many patients have a good response to oral or topical ketoconazole .
|
|