
Leiomyosarcoma
EPIDEMIOLOGY
Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs in all age groups, and there appears to be no gender predilection.
LEIOMYOSARCOMA AT A GLANCE
· Rare malignant tumor of smooth muscle: Cutaneous and subcutaneous types based on location of origin.
· Presentation: Enlarging cutaneous or subcutaneous tumor most commonly on hair-bearing areas of the lower extremities.
· Recurrence rate: High, with significant risk of metastases in case of subcutaneous leiomyosarcoma.
ETIOLOGY AND PATHOGENESIS
Leiomyosarcoma is a rare, malignant mesenchymal tumor of smooth muscle origin usually found in the uterus, the retroperitoneum, gastrointestinal tract, or deep soft tissue. The term superficial leiomyosarcomas refers to those tumors whose primary site of origin is the skin. Those derived from arrector pili or genital smooth muscles are termed cutaneous leiomyosarcomas, and those derived from blood vessel smooth muscle are termed subcutaneous leiomyosarcomas. In some cases, tumors have arisen in sites of earlier radiotherapy or trauma. Leiomyosarcomas typically arise de novo rather than from pre-existing leiomyomas.
CLINICAL FINDINGS
Leiomyosarcomas present as solitary, enlarging lesions most commonly on the hair-bearing area
of lower extremities. They can exhibit a variety of colors and may be painful, pruritic, or paresthetic. Cutaneous leiomyosarcoma usually presents as small (< 2 cm), sometimes ulcerated nodules that are fixed to the epidermis. Subcutaneous leiomyosarcomas tend to be larger and are usually not associated with epidermal change. Some patients have multiple grouped lesions; in one series, four of seven such patients had a previous retroperitoneal leiomyosarcoma, highlighting the importance of ruling out metastases in patients with numerous superficial leiomyosarcomas.
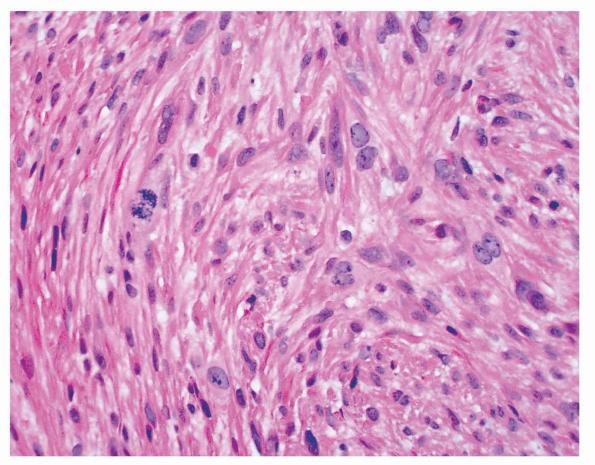
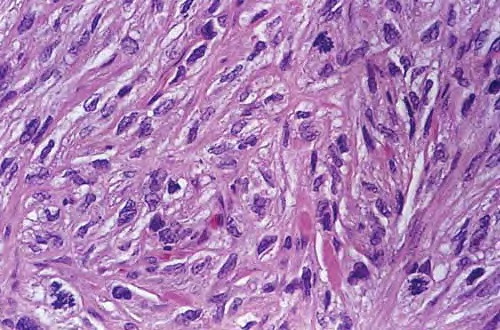
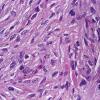
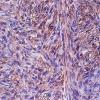
HISTOPATHOLOGY
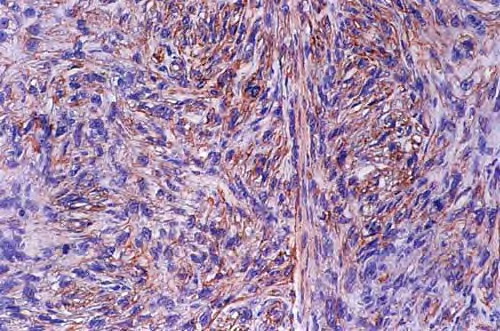
Leiomyosarcomas are large tumors consisting of smooth muscle fibers arranged in irregular, intersecting bundles and fascicles in the dermis and subcutis, often with infiltrating borders. Tumor cells exhibit smooth muscle differentiation with atypical cytologic features such as nuclear hyperchromasia, prominent nucleoli, mitosis, and necrosis . In less well-differentiated areas, highly pleomorphic and multinucleated cells may be found. Granular cell, epithelioid cell, myxoid, and sclerosing (or desmoplastic) variants have been described. Leiomyosarcomas must be histopathologically distinguished from other malignant cutaneous spindle cell tumors, such as spindle cell melanoma, spindle cell squamous cell carcinoma, or atypical fibroxanthoma. Leiomyosarcomas stain positive with smooth-muscle actin, desmin, and vimentin and occasionally with S100 and cytokeratin, which makes distinguishing them from melanoma and squamous cell carcinoma difficult in certain cases.
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of leiomyosarcoma includes any solitary, enlarging dermal or subcutaneous nodule: lipoma, dermatofibroma, dermatofibrosarcoma, neurofibroma, spindle cell melanoma, spindle cell squamous cell carcinoma, and atypical fibroxanthoma.
PROGNOSIS AND CLINICAL COURSE
The most important prognostic factor depends on whether the leiomyosarcoma is of cutaneous or subcutaneous origin. Although both cutaneous and subcutaneous lesions may recur locally in up to one-third to one-half of cases, the risk of metastasis is 5 percent to 10 percent for cutaneous leiomyosarcomas compared with 30 percent to 60 percent for subcutaneous leiomyosarcomas. The lung is the most common location of metastasis.
TREATMENT
Therapy for superficial leiomyosarcoma is wide local excision with 3- to 5-cm margins and re-excision for recurrent lesions. On acral locations, complete excision may require amputation. Patients with subcutaneous leiomyosarcomas should undergo
achest x-ray for metastases. Adjuvant radiation and/or chemotherapy has unclear benefit. Alternative local treatment modalities in selected patients include Mohs micrographic surgery, cryosurgery, and isolated limb perfusion with chemotherapeutic agents