|
Hydroa vacciniforme =المائية اللقاحينية |
 |
 |
 |
|
Hydroa Vacciniforme
HV is a very rare, intermittent, UVR-induced, blistering, scarring eruption of only some exposed skin, usually in children and only rarely in adults . The condition generally has onset by 10 years of age, with resolution by early adulthood. Usually sparse, occasionally coalescent, symmetrically scattered, sometimes hemorrhagic vesicles and bullae occurring within hairs of sun exposure are characteristic, particularly of the face, ears, and limbs. These umbilicate and crust over days, healing thereafter in weeks to leave persistent, disfiguring pock scars . Treatment is usually difficult. The restriction of UVR exposure and use of clothing cover are helpful, whereas the careful, regular application of high-protection, specifically broad-spectrum, sunscreens also has efficacy. In resistant cases, courses of prophylactic low-dose UVB phototherapy or PUVA are also helpful on occasion. All other therapies have seemed at best marginally useful.
|
|
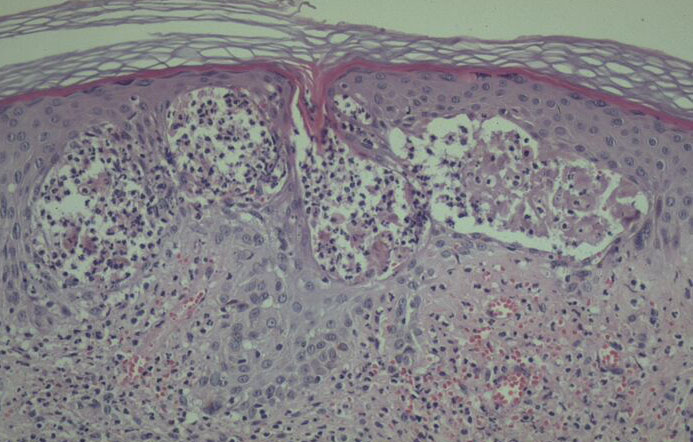
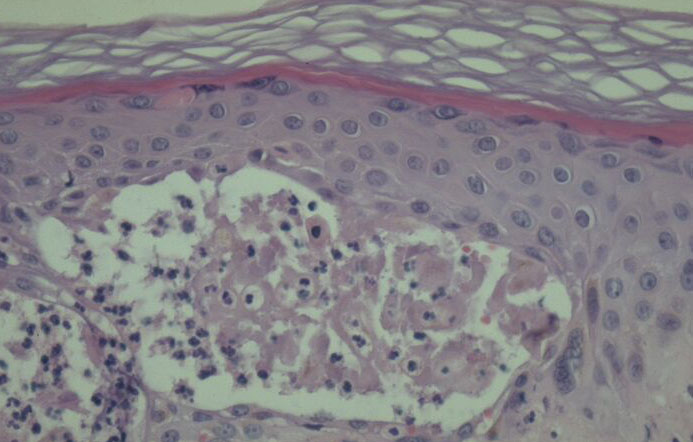
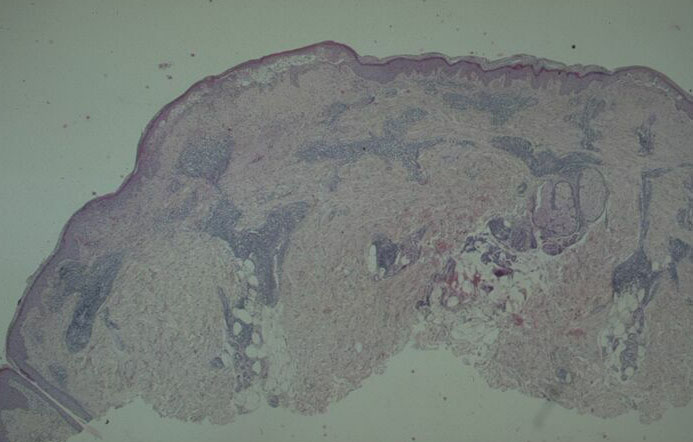
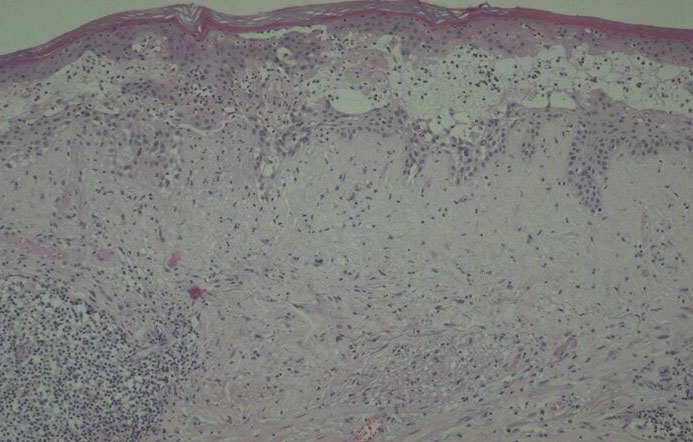
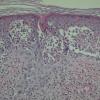
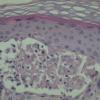
Histology.
The main, very characteristic, histologic abnormality is that of progressive intra- and intercellular epidermal edema leading to prominent reticular degeneration, vesiculation, and finally confluent epidermal necrosis . The vesicles contain fibrin and acute inflammatory cells and overlie a dermal cellular infiltrate of predominantly perivascular lymphocytes, histiocytes, and neutrophils . A vasculitis is not seen. In some cases, there is focal necrosis of the superficial dermis. Prominent secondary changes in late lesions may obscure the characteristic findings.
|
|
Pathogenesis.
The eruption of HV is clearly inducible by sunlight exposure, whereas artificial induction is more difficult, requiring repeated broad-spectrum or, less reliably, UVB skin exposure, but exact action spectra have not been determined . Blood, urine, and stool porphyrin concentrations, lesional viral studies, and circulating viral, antinuclear factor, and extractable nuclear antibody titers are normal. Further, the very PMLE-like clinical features of HV apart from its scarring and PMLE-like dermal perivascular mononuclear cell infiltration together strongly suggest similar pathogeneses for the two disorders; therefore, that HV may also be a DTH-type immunologic response to UVR-induced, endogenous, cutaneous autoantigen. In HV, however, the location of the putative antigen, the presence of a toxic photoproduct, or the intensity of the reaction may conceivably lead to the characteristic scarring.
|
|
Differential Diagnosis.
HV must be differentiated from cutaneous viral disorders, the porphyrias, lupus erythematosus; and the other idiopathic, probably immunologically based
|
|
photodermatoses by its clinical features and largely diagnostic histopathology, provided that appropriate viral studies, blood, urine, and stool porphyrin concentrations as well as circulating antinuclear factor and extractable nuclear antibody titers are also normal. The pattern of necrosis is remarkably similar to that seen in viral (including herpetic) infections and hand, foot, and mouth disease. Nevertheless, distinction from herpetic infection is easy,
as HV lesional biopsies lack viral inclusions, multinucleated keratinocytes, and nuclei with ground glass appearance; also, hair follicle necrosis is lacking. However, distinction from hand, foot, and mouth disease is more difficult, but the clinical settings of the two diseases are totally different. Finally, a T-cell lymphoma variant with facial necrotic lesions simulating HV has been described in Asian and native Central American Indian children and rarely in adults , but histologic distinction is not difficult, as atypical lymphoid cells are readily apparent in the lymphomatous infiltrate.
|
|
|
|
|