|
Granuloma Annulare
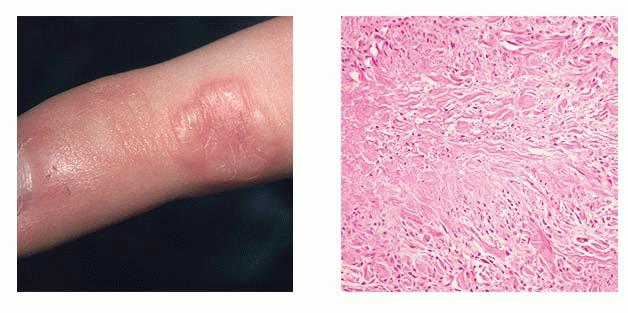
Granuloma annulare is an idiopathic, palisaded, granulomatous condition that is frequently encountered by dermatopathologists. It occurs most commonly in children and young adults but may affect all age groups. Females are affected somewhat more commonly than males. The lesions of granuloma annulare consist of small, firm, asymptomatic papules that are flesh colored or pale red and are often grouped in an annular or circinate fashion . There usually are several lesions, but there may be just one, or there may be many. The lesions are found most commonly on the arms, hands, legs, and feet. The trunk may also be involved, and rare sites of involvement include the palms, penis, ear, and periocular regions . Although chronic, the lesions usually subside after a number of years. Unusual variants of granuloma annulare include a generalized form,
consisting of hundreds of papules that are either discrete or confluent but only rarely show an annular arrangement perforating granuloma annulare, with umbilicated lesions occurring usually in a localized distribution and, rarely, in a generalized distribution erythematous or patch granuloma annulare, showing large, slightly infiltrated erythematous patches, with a palpable border, on which scattered papules may subsequently arise , and (d) subcutaneous/deep granuloma annulare, in which subcutaneous nodules occur, especially in children, either alone or in association with intradermal lesions . The subcutaneous nodules have a clinical appearance similar to that of rheumatoid nodules, although there is no history of arthritis, and there is a greater tendency to occur on the legs, feet, and, occasionally, the head
. In adults, similar lesions may be found near the small joints of the hands . A very rare, deep, destructive form of granuloma annulare has also been described .
A correlation between generalized papular granuloma annulare and diabetes mellitus has been observed by several authors . Granuloma annulare has been reported in at least 60 patients with HIV or AIDS, with a greater incidence of generalized disease in this population . Granuloma annulare-like lesions have also been reported to develop at sites of resolved herpes zoster and occasionally in association with tattoos , necrobiosis lipoidica , and sarcoidosis .
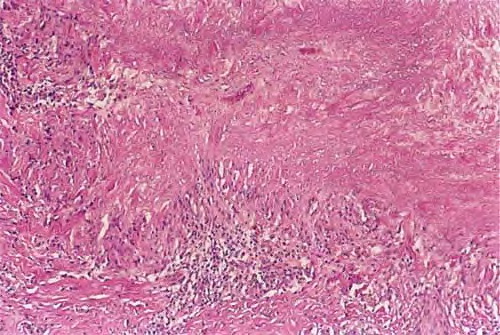
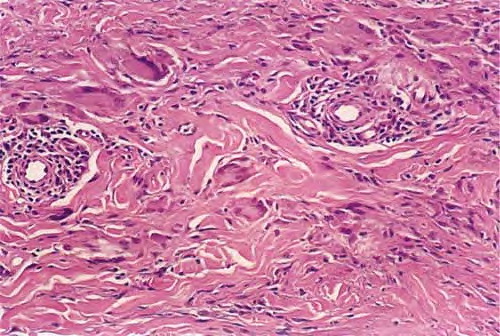
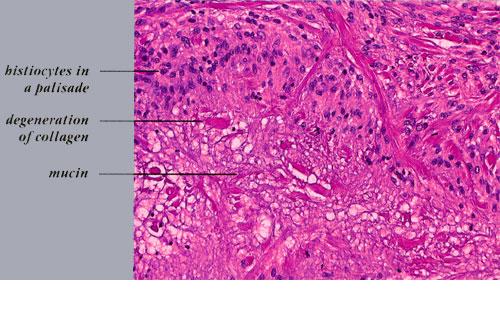
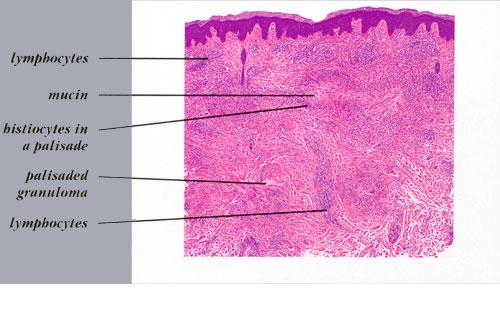
Histopathology.
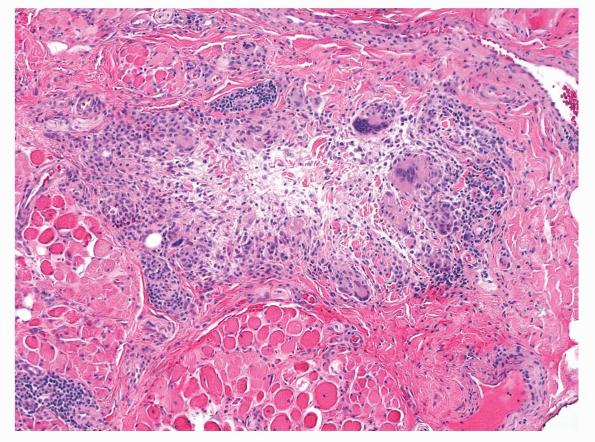
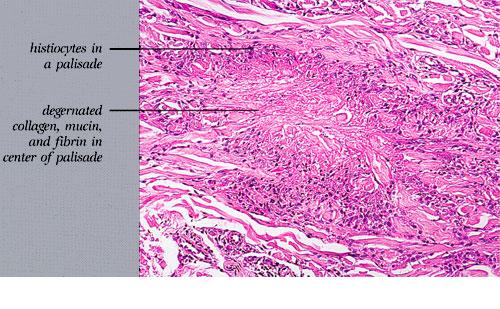
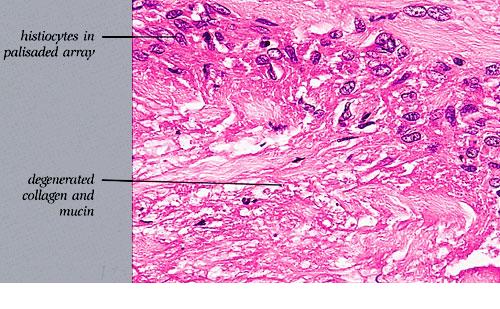
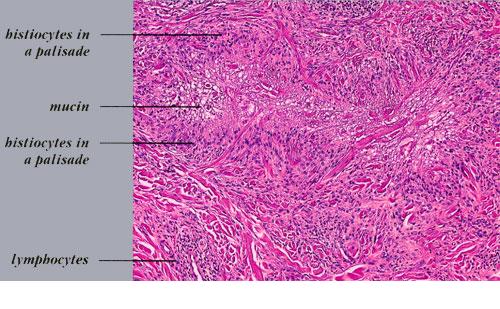
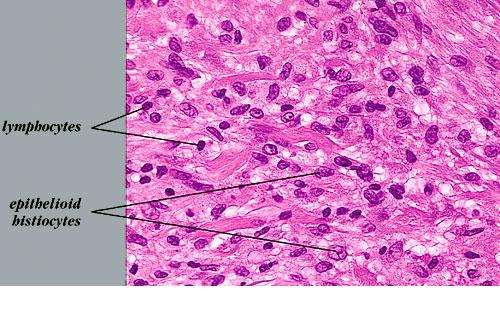
Histologically, granuloma annulare shows an infiltrate of histiocytes and a perivascular infiltrate of lymphocytes that is usually sparse. The histiocytes may be present in an interstitial pattern without apparent organization or in palisades surrounding areas with prominent mucin .Patterns between these two extremes occur, and typically a single biopsy will show histiocytes that are not palisaded, are slightly palisaded, and are well palisaded. Although degenerated collagen or small quantities of fibrin may be present , increased mucin is the hallmark of granuloma annulare. Increased mucin is almost always apparent on routinely stained sections as faint blue material with a stringy, finely granular appearance. Stains such as colloidal iron and Alcian blue can be used to highlight mucin if it is not clearly apparent. Occasionally, sections will not reveal increased mucin, particularly those lacking a palisaded arrangement of histiocytes. In biopsies with well-developed palisades, the central mucinous area is commonly accompanied by a few nuclear fragments or neutrophils. Plasma cells are present rarely. A sparse infiltrate of eosinophils is seen in approximately half of cases, and occasional biopsies show abundant eosinophils . Multinucleated histiocytes are present more often than not, but they are usually few and often subtle. They can occasionally be seen to have engulfed short, thick, blue-gray elastic fibers . The histiocytic infiltrate is usually present throughout the full thickness of the dermis or the middle and upper dermis, but occasionally just the superficial or the deep dermis is involved . Mitotic figures are usually rare (fewer than 1 per 10 high-power fields) but may be as frequent as 7 per 10 highpower fields in rare examples .
Rare examples of granuloma annulare show aggregates of epithelioid histiocytes, usually with some giant cells and a rim of lymphoid cells, which resemble the granulomas of sarcoidosis . These usually differ from sarcoidal granulomas, however, by showing poorer circumscription and by lacking asteroid bodies. Vascular changes in granuloma annulare are variable but generally inconspicuous . In some instances, however, there are fibrinoid deposits in vessel walls and occlusion of vascular lumina .
Among the variants of granuloma annulare mentioned, the usual histologic picture of palisaded and interstitial pattern is found in the generalized form . An interstitial pattern predominates in the erythematous and patch variants .
In perforating granuloma annulare, at least part of the palisading granulomatous process is located superficially and is associated with disruption of the epidermis
The subcutaneous nodules of deep granuloma annulare usually show large histiocytic palisades surrounding mucin and degenerated collagen . These central, degenerated foci exhibit a pale appearance ; however, examples in which mucin was not apparent or in which the central area appeared more fibrinoid have also been reported . Thus, subcutaneous granuloma annulare may be histologically indistinguishable from rheumatoid nodule, an appearance that has led to the term pseudorheumatoid nodule.
Pathogenesis.
The cause of granuloma annulare is unknown. Possible precipitating events in small subsets of patients have included insect bites, warts, erythema multiforme, herpes zoster, exposure to sunlight, hepatitis B vaccine, andtuberculin skin tests . There is likely an increased incidence and increased disease severity in patients with diabetes mellitus. Thrombi or vasculitic changes have been noted in some examples, and it is possible that what we term granuloma annulare may represent a variety of disease processes.
Electron microscopic examination reveals degeneration of both collagen and elastic fibers in granuloma annulare . The macrophages (histiocytes) show a high content of primary Iysosomes and considerable cytoplasmic activity with release of lysosomal enzymes into the extracellular space . Synthesis of types I and III collagen also occurs, probably as a reparative response . A cell-mediated immune response also appears to be involved, marked by prominent activated helper T cells . One immunoperoxidase study of the histiocytic population showed staining for lysozyme but not for other macrophage markers such as HAM 56 or CD6B . Another demonstrated positivity for these two markers .
|