
Mammary and Extramammary
Paget Disease
EPIDEMIOLOGY
Mammary Paget disease (MPD) represents approximately 1 percent to 3 percent of breast neoplasms. The peak incidence is between 50 and 60 years of age. MPD in males is extremely rare; almost all reported cases occur in women.
Extramammary Paget disease (EMPD) is a rare neoplasm that affects apocrine gland-bearing skin, such as the vulva, perianal region, scrotum, and penis. The majority of patients are women in the sixth through eighth decades of life. The vulva is the most commonly affected area, and EMPD represents 2 percent of all vulval malignancies.
ETIOLOGY AND PATHOGENESIS
MPD is almost always associated with underlying in situ or invasive intraductal adenocarcinoma of the breast (up to 98 percent of cases in some studies). Malignant cells directly extend from the underlying tumor into the epidermis via the lactiferous ducts. Rare cases are reported to have originated primarily in the epidermis of the nipple.
Unlike MPD, in which almost all cases have a documented underlying neoplasm, EMPD does not have a uniform histogenesis, and several different forms have been described. Primary EMPD is the most common type and accounts for the majority of all patients with this disease. Underlying carcinoma is not present, and these cases represent a primary intraepithelial neoplasm. The malignant cells are thought to originate from intraepidermal apocrine glands or from pluripotential cells of the epidermis. The neoplasm can then invade the dermis and metastasize via lymphatic spread. In contrast, a smaller proportion of EMPD cases are associated with an underlying apocrine carcinoma or internal malignancy (secondary EMPD). These cases are due to epidermotropic spread of malignant cells from the underlying tumor. Approximately 15 percent of cases are associated with an underlying internal carcinoma. The most common visceral malignancies associated with EMPD are carcinomas of the rectum, bladder, urethra, cervix, and prostate.
CLINICAL FINDINGS
History
Both MPD and EMPD often present with a long-standing history of pruritic, erythematous, scaly patches on the breast and in the groin, perineum, and axilla, respectively. Frequently there is a delay in diagnosis of many months to years as treatment with topical steroids and antifungal agents for presumed inflammatory or infectious dermatitis are initiated. After continued failure to respond to these medications, a diagnostic biopsy is ultimately performed.
Cutaneous Lesions
MPD frequently presents as a unilateral, erythematous, scaly plaque or patch involving the nipple and occasionally the areola . Ulceration and weeping with an eczematous appearance is frequently present. Nipple erosion and discharge may occur. Retraction of the nipple can be seen. Pain, burning, and pruritus are frequently reported by patients.
Lesions of EMPD are clinically similar to MPD and often present as a well-defined, moist, erythematous, scaly, eczematous patch. Hypo- and hyperpigmentation can occur. Burning and intense pruritus are commonly reported. Lesions typically involve apocrine gland-bearing skin (i.e., groin and axilla); the most frequent site is the vulva, but perineal, scrotal , perianal , and penile skin are also common areas. Rarely, ectopic EMPD has been reported in areas that are relatively free of apocrine glands, such as the chest, abdomen, thigh, eyelids, face, and external auditory canal.7-11 Given the unclear association with underlying carcinoma in EMPD as compared to MPD, a palpable mass is much less frequently found on examination.
Differential Diagnosis of Mammary (MPD) and Extramammary Paget Disease (EMPD)
|
|
Most Likely
|
Consider
|
Always Rule Out
|
|
MPD
|
Nipple eczema
|
Hailey-Hailey disease
|
Bowen disease
|
|
|
Erosive adenomatosis
|
Pemphigus
|
Basal cell carcinoma
|
|
|
Psoriasis
|
|
Malignant melanoma
|
|
|
Dermatophyte infection
|
|
|
|
EMPD
|
Candidiasis
|
Lichen sclerosus et atrophicus
|
Bowen disease
|
|
|
Tinea cruris
|
Pemphigus
|
Erythroplasia of Queyrat
|
|
|
Psoriasis
|
Lichen simplex chronicus
|
Malignant melanoma
|
|
|
Seborrheic dermatitis
|
Lichen planus
|
|
|
|
Nummular dermatitis
|
Drug eruption
|
|
Related Physical Findings
Up to one-half of all patients with MPD have a palpable underlying breast mass.4,5,12,13 Of those patients with a palpable underlying tumor, half have axillary adenopathy due to lymph node metastasis.4,5 Palpable lymph nodes are much less frequently present in EMPD. Complete physical examination is required in all cases of MPD and EMPD for indications of metastases and underlying malignancy. Patients may present with symptoms and physical findings associated with any underlying carcinoma.
Laboratory Tests
PATHOLOGY
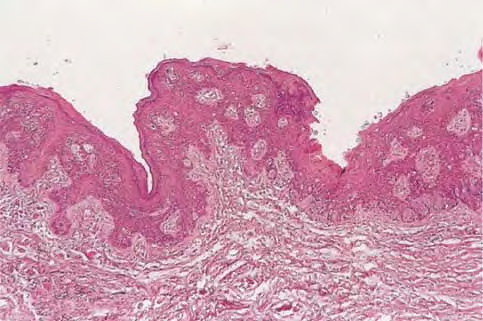
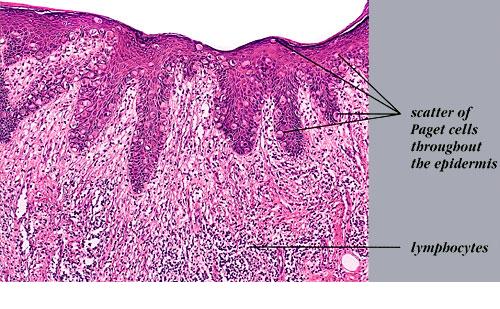
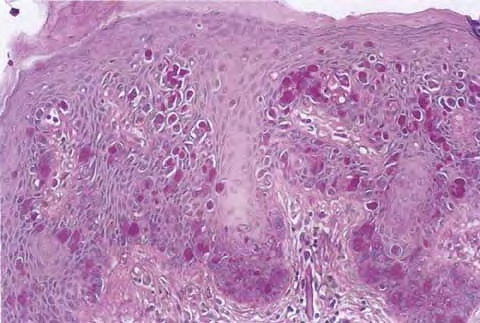
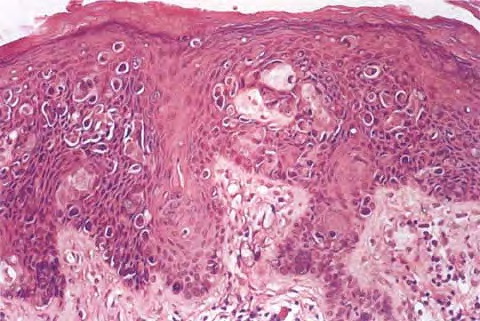
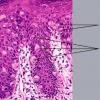
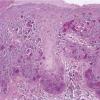
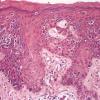
The intraepidermal adenocarcinoma of EMPD and MPD has a similar histologic appearance. There are groups, clusters, or single cells within the epidermis that show nuclear enlargement with atypia, prominent nucleoli, and well-defined ample cytoplasms . Intercellular bridges are absent. The cells can be within all levels of the epidermis and can compress but preserve the basal layer without junctional nest formation. The cells can extend into the contiguous epithelium of hair follicles and sweat gland ducts. Acanthosis, hyperkeratosis, and parakeratosis are often present. These cells have a “pagetoid” appearance and simulate other intraepidermal malignancies, including melanoma, pagetoid squamous cell carcinoma in situ, mycosis fungoides, cutaneous adnexal carcinomas (sebaceous carcinoma, porocarcinoma, and others), Merkel cell carcinoma, Langerhans cell histiocytosis, and other epidermotropic cutaneous metastases. The cells of MPD and EMPD can be pigmented, which should not necessarily indicate they are melanocytic.
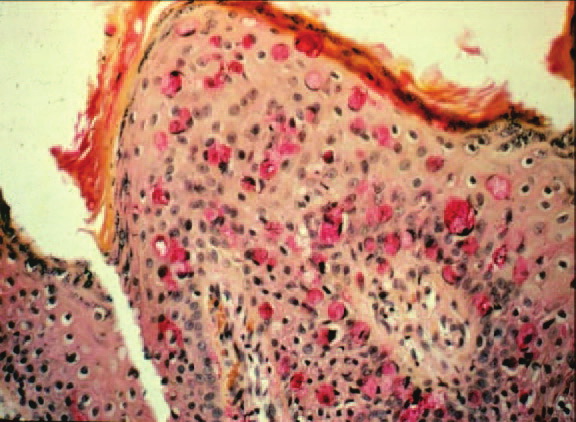
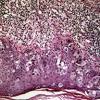
Paget's cells have intracellular mucopolysaccharides, with EMPD having a greater amount of mucin as compared
to MPD. As a result, cells frequently show positive staining for periodic acid-Schiff and diastase resistance, mucicarmine, Alcian blue at pH 2.5, and colloidal iron . However, there are can be focal “skip areas” that are devoid of mucin, resulting in negative stains.
Immunohistochemistry is a useful adjunct in making the correct diagnosis. Low-molecular-weight cytokeratin stains cytokeratin 7 (CK7) and anti-cytokeratin (CAM 5.2) are sensitive markers for both MPD and EMPD . They are not completely specific, however, with both Toker and Merkel cells showing CK7 positivity. The cells of MPD and EMPD may stain with carcinoembryonic antigen and epithelial membrane antigen. The most useful keratin markers for Paget disease are CAM 5.2 and CK7, as they stain more than 90 percent of Paget's cells but do not react with epidermal or mucosal keratinocytes.13,14 The cells of pagetoid squamous cell carcinoma in situ typically do not stain with CK7 and CAM 5.2. S100 and HMB-45 are useful markers to exclude melanoma, as both are typically negative in MPD and EMPD.
CK20 positivity has been found more frequently in cases of secondary EMPD with underlying carcinoma as compared to those cases of primary intraepithelial EMPD (CK7+/CK20-).15
Gross cystic disease fluid protein-15 (GCDFP-15) is a marker for apocrine epithelium and is typically positive in primary EMPD not associated with underlying neoplasm. In contrast, GCDFP-15 is frequently negative in those cases of secondary EMPD with an associated malignancy.16
Mucin core protein (MUC) expression is useful in the diagnosis of MPD and EMPD.17 MUC1 positivity is noted in both MPD and EMPD. MUC2 expression is generally negative in primary EMPD, but may be expressed in those cases of secondary EMPD with an associated underlying gastrointestinal adenocarcinoma. MUC5AC is frequently positive in primary EMPD and less commonly noted in secondary EMPD or those cases of primary intraepithelial EMPD that becomes invasive.
SPECIAL TESTS
Diagnosis of MPD and EMPD should be accompanied by a thorough search for underlying malignancy. Mammography is indicated in all cases of MPD, with biopsy of any underlying breast mass.
In cases of EMPD, workup is directed toward the possibility of an underlying gastrointestinal or genitourinary neoplasm. Imaging of the abdomen and pelvis, colonoscopy, barium enema, cystoscopy, intravenous pyelogram, chest x-ray and mammogram (for the rare association of EMPD and MPD), and blood work are appropriate tests. Some reports have suggested that positron emission tomography scans may be useful for cases of invasive EMPD to evaluate for lymph node involvement and metastases.
COMPLICATIONS
Failure to identify and adequately treat cases of MPD can lead to metastatic disease with a poor prognosis. EMPD, if left untreated, can become invasive with a less favorable outcome.
PROGNOSIS AND CLINICAL COURSE
Overall survival in patients with MPD is affected by lymph node status and the presence of an underlying breast mass. Patients with negative lymph nodes have been shown to have a 10-year survival rate of 75 percent to 95 percent, whereas those with positive lymph nodes have a survival rate of 20 percent to 45 percent.4 Patients with a palpable breast mass have a 5-year survival probability of 35 percent to 51 percent, as compared to 75 percent to 82 percent in patients without a palpable mass.
The prognosis for primary EMPD confined to the epidermis is excellent with appropriate treatment. Careful monitoring for early detection of local recurrence is critical given the multifocal pattern often present in EMPD. In contrast, invasive EMPD has a high rate of metastasis and carries a poor prognosis. The depth of invasion appears to be an important prognostic factor, with microscopic invasive disease (less than 1 mm) having a more favorable prognosis as compared to those with deeper invasion. Lymphovascular invasion and regional lymph node metastases markedly reduces overall survival rate and indicates a very poor prognosis. Clitoral EMPD has been shown to have a higher incidence of death from the disease as compared to other vulvar EMPD locations. In cases of secondary EMPD, the prognosis is related to the underlying carcinoma.
TREATMENT
Mammary Paget Disease
Treatment of MPD is surgical. However, optimal surgical management of MPD remains to be defined, and treatment choice is frequently based on the presence or absence of an underlying breast mass. Mastectomy remains the standard definitive treatment. However, evidence suggests that MPD treated with breast-conserving surgery results in local control and survival rates similar to those achieved with mastectomy. Proper preoperative imaging is required to rule out multi-focal disease that would make breast-conserving therapy less effective and favor mastectomy. Lymph node evaluation via axillary dissection or sentinel lymph node biopsy must be considered in MPD. Adjuvant therapy with radiation, chemotherapy, or hormonal therapy is recommended based on lymph node status and specific features of the primary tumor. All diagnoses of MPD require referral to a physician with expertise in the management of breast cancer.
Extramammary Paget Disease
EMPD has been treated with a variety of different modalities. Although surgical management of the disease is the most frequently used method, various other treatments have a role for non-surgical candidates and as adjuvant therapy.
SURGERY
Surgery remains the treatment of choice for EMPD when tolerated by the patient. However, high local recurrence rates are seen after standard surgical excision, even with wide margins. This is most likely due to the irregular margins, multi-focal nature of the condition, and subclinical involvement of apparently unaffected skin.
Several reviews have shown an overall recurrence rate of up to 44 percent with wide local excision, The local recurrence rates are higher in cases of invasive disease as compared to those limited to intraepithelial involvement. In addition, more radical and extensive surgeries are associated with lower rates of local recurrence. Patients with primary vulvar EMPD treated with radical vulvectomy, radical hemivulvectomy, and wide local excision have reported recurrence rates of 15 percent, 20 percent, and 43 percent, respectively.
Multiple scouting biopsies to help delineate the extent of the disease before surgery can be a useful adjuvant technique.26 Intraoperative staining with CK7 is the preferred immunostain for intraoperative tissue evaluation.27 Sentinel lymph node biopsy has been described in the treatment of EMPD. Although this technique has been limited to a small number of reported patients and most cases of EMPD have in situ disease, sentinel lymph node biopsy may prove beneficial for those patients with increased risk of lymph node involvement and metastasis (i.e., dermal invasion of Paget's cells).29
MOHS MICROGRAPHIC SURGICAL EXCISION
Given the high rates of local recurrence and the significant morbidity associated with radical and repeated surgeries, Mohs micrographic surgical excision (MMS) has been used to improve cure rates and for tissue sparing of critical genitourinary anatomic structures as compared to wide local excision.2,27,30,31 The recurrence rate after treatment with MMS has been reported as 16 percent for primary EMPD and 50 percent for recurrent EMPD. Ninety-seven percent of the cases treated with MMS required margins of 5 cm from the clinical tumor margin. However, if surgical margins of only 2 cm were used, as may be the case because wider margins may not be feasible when operating on the genitalia, only 59 percent of
the tumors would have been cleared. The 40 percent expected recurrence rate with 2-cm margins is consistent with what is seen in various reports of EMPD treated with standard wide excision. This further validates a potential benefit of frozen horizontal sectioning to evaluate 100 percent of the surgical margin and reduces the possibility of residual tumor, which may result from narrow margins in standard excision.
RADIOTHERAPY
Although surgery remains the traditional treatment for EMPD, radiotherapy may be indicated in those patients who are poor surgical candidates or are concerned with the morbidity of genitourinary function due to extensive surgery that is often required for curative treatment.32, 33, 34 In addition, radiotherapy has been described as useful for local recurrence after surgery or as an adjuvant therapy in those patients with a high risk of recurrence.34,35 No randomized controlled studies comparing surgery to radiotherapy have been performed to date.
TOPICAL CHEMOTHERAPY AND IMMUNOMODULATORS
Topical agents, including 5-fluorouracil (5-FU) and imiquimod, have been used to treat EMPD with varying degrees of success.
5-FU may be useful as a preoperative adjunctive treatment to highlight the subclinical extent of disease before MMS or for early postoperative detection of recurrence.36 However, topical 5-FU has not proven to be a reliably curative agent in the treatment of EMPD.37 This is likely due to the limited penetration of the drug and the inability to reach the deeper epidermal layers and adnexal structures that are frequently involved in EMPD.
Imiquimod has been reported to result in clinical and histologic cure in several case reports.38-42 Given the limited number of patients treated with this medication, further studies and long-term follow-up in a larger cohort is necessary.
SYSTEMIC CHEMOTHERAPY
Systemic chemotherapy has been used to treat patients with invasive and metastatic disease and may be considered in rare cases in which surgery and radiotherapy are contraindicated. Limited reports of systemic chemotherapy for the treatment of EMPD have been described, including a combination of low-dose 5-fluorouracil and cisplatin43; a combination of 5-FU, cisplatin, mitomycin C, epirubicin, and vincristine and docetaxel.
PHOTODYNAMIC THERAPY
Given the patchy nature of EMPD and extension beyond clinically visible tumor, photodynamic therapy (PDT) is a potentially useful treatment modality. Although the limited number of studies and reports makes further investigation necessary, PDT may be considered in patients who are poor surgical candidates, are at risk for significant functional morbidity due to the anatomic location of the disease, or have recurrent postsurgical disease.48-51 Limiting treatment to intraepithelial disease is prudent given the limitations of current PDT technology. PDT has been described as an adjuvant to surgical treatment to better define clinical margins and improve recurrence rates.27
PREVENTION
Both EMPD and MPD are not preventable diseases. Rather, early diagnosis is the key to a favorable prognosis, and any unilateral eczematous rash on the breast or in the groin that does not respond to an appropriate course of topical treatment warrants a biopsy. Routine mammography may allow early detection of underlying breast carcinoma in women of appropriate screening age.