ERYTHEMA NODOSUM
LEPROSUM
ENL occurs most often in LL, in up to 75 percent of cases, but is not rare in BL patients. It is important to appreciate that ENL is not erythema nodosum occurring in leprosy; it is a leprosy-specific response, which has some features in common with erythema nodosum . It may occur before, during, or after chemotherapy. The median time of onset is almost 1 year after onset of treatment. Clinically, this reaction is characterized by crops of painful and tender bright-pink, dermal and subcutaneous nodules arising in clinically normal skin, in association with fever, anorexia, and malaise .Lesions may be targetoid, vesicular, pustular, ulcerative, or necrotic. Of the other organs involved, arthralgias and arthritis are more common in ENL than are neuritis, adenitis, orchitis/epididymitis, or iritis, but each may rarely be the initial presentation. Involvement of both upper and lower extremities is the rule, and facial lesions occur in one-half of the patients. A neutrophilic leukocytosis is often present, occasionally leukemoid in degree. Severe episodes can be associated with an abrupt fall in hematocrit, up to 5 g/dL, easily mistaken for dapsone-induced hemolysis. The improvement in response to thalidomide is dramatic in greater than 90 percent of patients, perhaps qualifying as a diagnostic criterion. When ENL is the presenting mode of leprosy, there may be little or no stigmata of the underlying multibacillary disease. ENL may be precipitated by pregnancy or pyogenic infections.
Although episodes of ENL may be occasional or sporadic, in the more severely involved patients, episodes can be frequent to virtually unremitting. In the latter, brawny induration of the anterior thighs and lateral portion of the arms is characteristic, perhaps a reversible fibrosis. The course of ENL may be
prolonged, and the median required duration of anti-inflammatory treatment is approximately 5 years.
The diagnosis of ENL, if considered, is usually not difficult, as the clinical and histologic features are characteristic and the response to thalidomide is often dramatic.
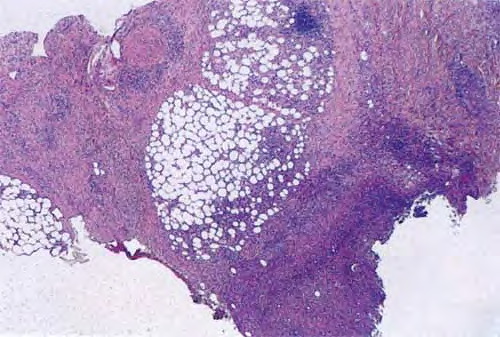
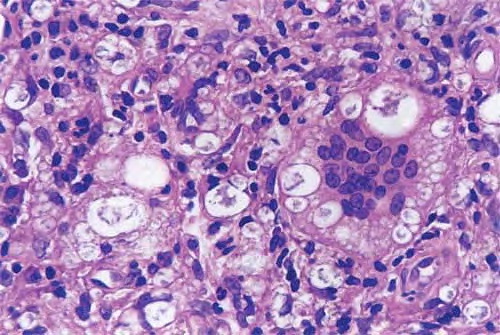
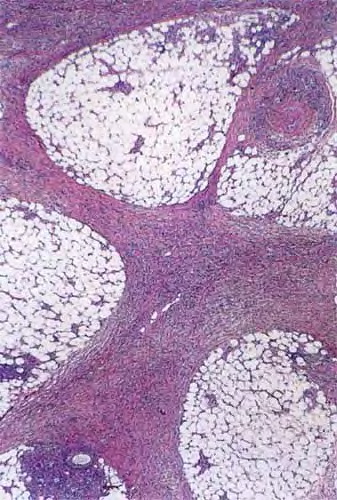
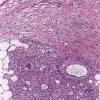
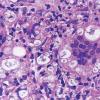
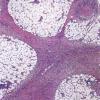
Histopathologically, the signature cell of ENL is the neutrophil, which may be abundant, scant, or absent, if an old lesion is sampled . Other common features include an increase in lymphocytes, a thickened epidermis, and a lobular panniculitis. Vasculitis is uncommon. The usual histologic pattern is a “bottom heavy” infiltrate, preferring the deep dermis and subcutis.