|
Erythema Nodosum
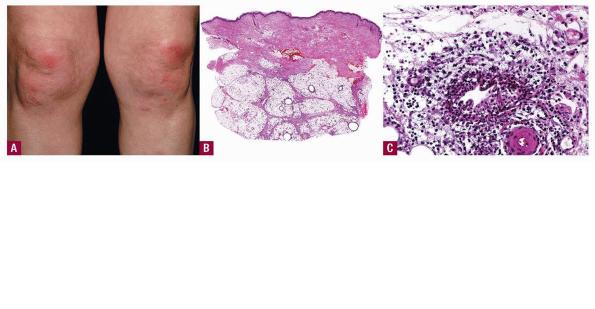
Clinical Presentation. An acute form and a chronic form of erythema nodosum exist, which differ in their clinical manifestations but do not have uniformly recognized differences in their histologic characteristics .
|
|
In the acute form of erythema nodosum, there is a sudden appearance of tender, bright red or dusky red-purple nodules to plaques that only slightly elevate the level of the skin surface . The lesions vary from 1 to 5 cm in diameter and have a strong predilection for the anterior surfaces of the lower legs, although they may occur elsewhere, especially on the calves, thighs, and, in severe cases, on the forearms, hands, and even the face. They occur mostly on the dependent regions of the body and tend to be distributed symmetrically. The lesions do not ulcerate and generally involute within a few weeks without leaving a depressed scar. As a result of the intermittent appearance of new lesions, the disease may persist for several months. The acute disease often is accompanied by fever, malaise, leukocytosis, and arthropathy . The lesions are tender and warm. Lesions near a joint can mimic an arthritis. Focal hemorrhages are common and can cause the lesions to resemble bruises (erythema contusiforme), even to changing in color from red to purple and on to green and blue, as they age and resolve. Bilateral hilar adenopathy can be present in patients with acute erythema nodosum without sarcoidosis since a number of pulmonary infections can produce both hilar adenopathy and erythema nodosum. Erythema nodosum occurs in 10% to 20% of patients with sarcoidosis and is thought to portend a good prognosis .
|
|
The chronic form of erythema nodosum is also known as erythema nodosum migrans or subacute nodular migratory panniculitis of Vilanova and Pinol . There are one or several red, subcutaneous nodules that are found, usually unilaterally, on the lower leg. Vilanova observed that almost all of the patients were women (16 to 65 years of age) with a solitary lesion and a recent history of sore throat and arthralgia. Tenderness is slight or absent. The nodules enlarge by peripheral extension into plaques, often with central clearing. The duration may be from a few months to a few years.
|
|
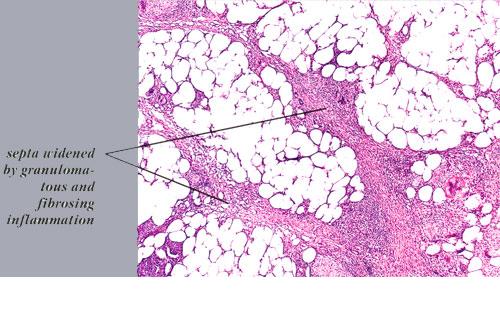
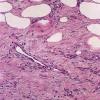
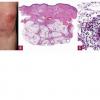
Histopathology. The histologic changes are present mainly in and near the septa of the subcutaneous tissue .
|
|
. The overlying dermis often has only a minimal to moderate, superficial and deep perivascular lymphocytic infiltrate.
|
|
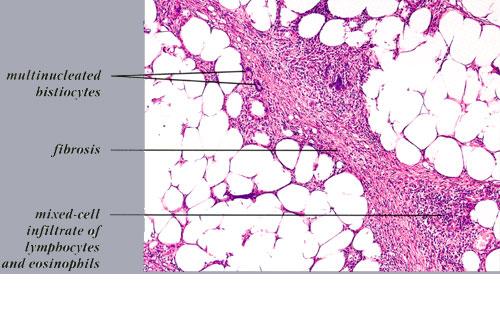
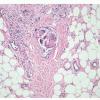
In the early lesions of acute erythema nodosum, there is edema of the septa with a Iymphohistiocytic infiltrate, having a slight admixture of neutrophils and eosinophils . Focal fibrin deposition and extravasation of erythrocytes occur frequently and can be revealed by spectral microscopy . Often, the inflammation is most intense at the periphery of the edematous septa and extends
|
|
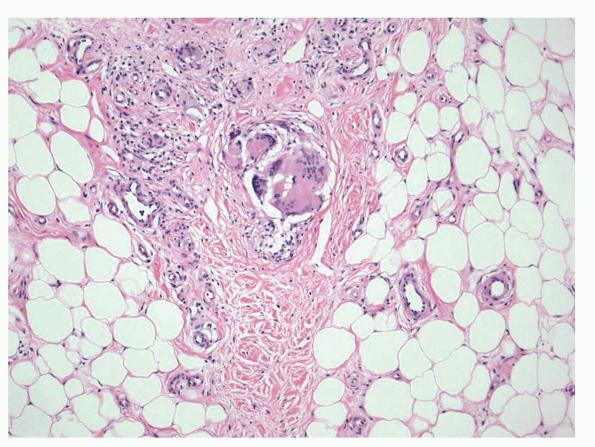
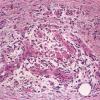
into the periphery of the fat lobules between the individual fat cells in a lacelike fashion. Necrosis of the fat is not prominent. Rarely, clusters of neutrophils are present or the infiltrate is predominantly neutrophilic . Clusters of macrophages around small blood vessels, or a slitlike space, occur in early lesions and are known as Miescher's radial nodules . Some authors have failed to find central vessels and have considered Miescher's nodules to be characteristic of erythema nodosum, stating that they can be found in all stages of erythema nodosum . The degree of vascular involvement is variable . Usually, there is edema of the walls of veins with separation of the muscular layers . Infiltration by lymphocytes is common, but neutrophils and eosinophils can be present as well. Necrosis of the vessel walls is very rare but has been observed in a few patients with lesions clinically indistinguishable from erythema nodosum . For example, focal vasculitis has been found in a few patients with acute erythema nodosum secondary to infections and in a few cases of recurrent
|
|
erythema nodosum that is secondary to medications or estrogenic oral contraceptives.
|
|
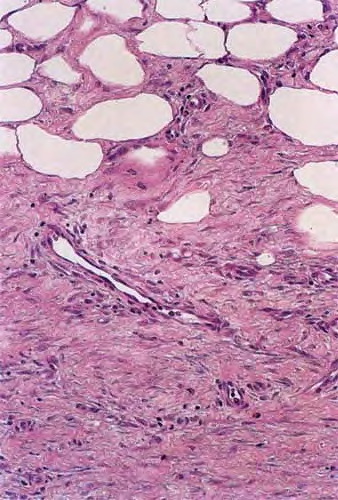
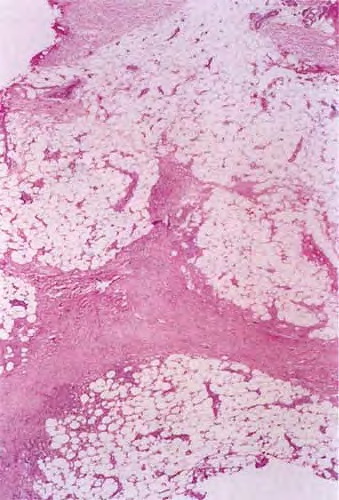
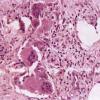
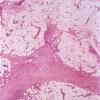
Later lesions of acute erythema nodosum show widening of the septa, often with fibrosis and with inflammation at the edges of the septa and involving the periphery of the fat lobules . Neutrophils usually are absent, and the vascular changes are less prominent than in early lesions. There are more macrophages in the infiltrate. Macrophages at the edges of the fat lobules show phagocytosis of lipid from damaged adipocytes, and the small droplets of lipid in their cytoplasm give them a "foam cell" appearance. Granulomas formed by macrophages, without lipid deposition, are more frequent
|
|
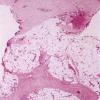
when late lesions are compared with early ones . The granulomas often are loosely formed with macrophages predominating in a focus with multinucleated giant cells. Occasionally, well-formed, discrete sarcoidal granulomas occur in small numbers in the septa. The multinucleated cells usually have an irregular distribution of the nuclei in the cytoplasm. The oldest lesions have septal widening and fibrosis with a decrease in all of the inflammatory cells.
|
|
In chronic erythema nodosum, the histologic findings are generally similar to those of the late stages of acute erythema nodosum. However, granulomas and lipogranulomas often are more pronounced in chronic erythema nodosum. There is vascular proliferation and thickening of the endothelium with extravasation of erythrocytes . In some instances, numerous well-formed granulomas can be found and consist of epithelioid macrophages and giant cells without caseous necrosis . Although significant degrees of vasculitis have been observed by some authors , others have found vascular changes to be slight or absent . The presence of thickened fibrotic septa with marked capillary proliferation and massive granulomatous reaction have led several authors to consider erythema nodosum migrans as an entity separate from the late lesions of acute erythema nodosum . Other authors consider all of these histologic patterns to be included within the spectrum of chronic erythema nodosum .
|
|
Pathogenesis.
Although the cause of erythema nodosum cannot always be determined in an individual patient, streptococcal infection is the most common among the known causes, especially in children, as evidenced by elevation of antistreptolysin a titers. The diseases that can be associated with erythema nodosum are numerous and have been reviewed recently . In short, they may be divided into the following: infections with bacteria, fungi, or protozoa; viral diseases; malignancies; medications; and miscellaneous conditions. The most frequent bacterial infections are streptococcal infection, tuberculosis, Yersinia enterocofitica infection , brucellosis, leptospirosis, tularemia, Chlamydia infection, and Mycoplasma pneumoniae infection. The most frequently associated fungal infections are coccidioidomycosis, histoplasmosis , dermatophytosis, aspergillosis, and blastomycosis, depending on the geographic location and immune status of the patient. Protozoal infections such as toxoplasmosis, amoebiasis, and Giardia infection can cause erythema nodosum. Among the associated viral and rickettsial infections are herpes simplex, infectious mononucleosis (due to Epstein-Barr virus infection), lymphogranuloma venereum, ornithosis, and psittacosis. Erythema nodosum occurs with some cases of leukemia, Hodgkin's disease, and non-Hodgkin's lymphomas, as well as with some other cancers, particularly after irradiation or other treatment releases antigens into the circulation by tumor necrosis. Among the miscellaneous associations are several diseases that can cause considerable difficulty in diagnosis, particularly acute sarcoidosis, which can have erythema nodosum as part of a symptom complex along with slight hilar adenopathy, fever, arthralgias, and occasionally acute iritis, uveitis, and parotid swelling (uveoparotid fever). The sarcoidal granulomas that can occur in erythema nodosum are less frequent, are septal in location, and are associated with edema, in contrast to the abundant granulomas that occur in subcutaneous sarcoidosis, without much edema and mostly in the lobules of the subcutaneous fat. Likewise, Crohn's disease can be associated with erythema nodosum (1 D), and the two diseases can be difficult to distinguish from each other histologically in the skin involvement unless there is ulceration, which does not occur in erythema nodosum . Other associated conditions are ulcerative colitis, and Behcet's disease (29). The panniculitis in Behcet's disease may resemble erythema nodosum clinically but often is different histologically in having neutrophilic and
|
|
lymphocytic vasculitis, which is predominantly lobular in distribution (3D). Erythema nodosum and Sweet's syndrome have been reported in the same patient . Among the many medications that can cause erythema nodosum, the most common ones are sulfonamides, estrogens, and oral contraceptives . There are rare associations with aminopyrine, antimony compounds, arsphenamine, bromides, iodides, phenacetin, salicylates, immunizations, and vaccinations . Such a great diversity in inciting agents and circumstances suggests that several mechanisms may be capable of triggering the clinical and histopathologic changes that are classified as erythema nodosum.
|
|
Direct immunofluorescence studies have shown deposits of immunoglobulins only very rarely in the blood vessel walls in erythema nodosum . Small amounts of complement in the vessel walls and abundant fibrin around the vessels are frequent but nonspecific findings. On electron microscopic examination, nonspecific vascular changes consisting of damage to endothelial cells and lymphocytic infiltration have been described .
|
|
The occurrence of erythema nodosum as a response to medications and to tuberculin skin testing in patients with a positive reaction suggest that a type IV delayed hypersensitivity reaction may play an important role, especially given the paucity of reports of immunoglobulin deposition and the usual failure to detect circulating immune complexes (34). However, in some patients, a type III immune complex reaction could be responsible. Circulating immune complexes and rheumatoid factors have been detected in some patients with sarcoidosis and erythema
|
|
nodosum . In approximately 50% of cases, there is no cause identified . The predilection for the anterior shins and for dependent parts of the body suggests that trauma or sluggish blood flow playa role in the localization of the lesions, but other factors such as the distribution of immunoreactive macrophages and dendritic cells need investigation as well.
|
|
Differential Diagnosis.
Erythema nodosum needs to be distinguished from erythema induratum and nodular vasculitis. Vasculitis and zones of fat necrosis are absent in erythema nodosum and frequent in erythema induratum. In patients suspected to have erythema nodosum but with necrotizing vasculitis, the possibility of cutaneous polyarteritis nodosa must be considered. In the latter disease, medium-sized arteries rather than veins or small-caliber blood vessels are affected, with necrosis of the walls of affected arteries. In contrast, nodular vasculitis has mainly lymphocytic infiltration with fibrous thickening and obliteration of vascular lumens. Superficial migratory thrombophlebitis, unlike erythema nodosum, has a large vein containing thrombus in the center of the lumen. Syphilitic gummas are ulcerative irregular granulomatous lesions that produce depressed scars. Subcutaneous tuberculosis can mimic erythema nodosum in lesions that are extending from underlying organs, soft tissues, or bone. Stains for acid-fast organisms and cultures are needed. Subcutaneous tuberculosis can spare the upper portion of the panniculus, whereas erythema nodosum does not. Erythema nodosum does not have granulomas or sclerosis in the overlying dermis, and in this way can be distinguished from most cases of sarcoidosis, scleroderma, necrobiosis lipoidica diabeticorum, ruptured follicular cysts, and factitial traumatic panniculitis.
|
|