|
Epidermolytic Hyperkeratosis =انحلال البشرة مفرط التقرن |
 |
 |
 |
|
Epidermolytic Hyperkeratosis
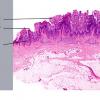
Epidermolytic hyperkeratosis, an autosomal dominantly inherited disease also known as bullous congenital ichthyosiform erythroderma, shows generalized erythema from the time of birth . Within a few days after birth, there is thick, brown, verrucous scaling . The flexural surfaces of the extremities show marked involvement, often consisting of furrowed hyperkeratosis. Vesicles and bullae and erosions are usually encountered only during the first few years.
|
|
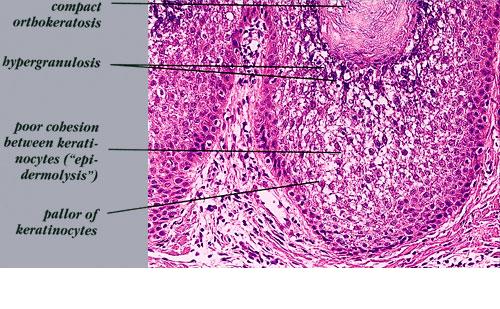
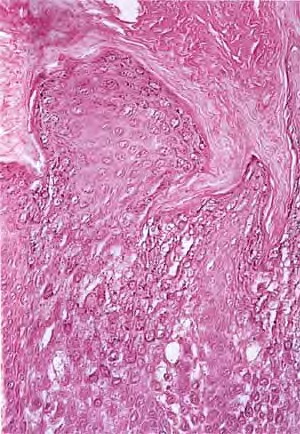
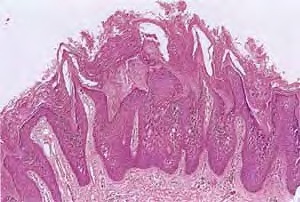
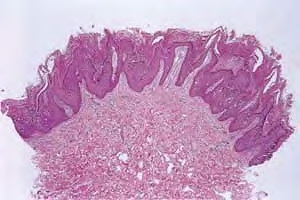
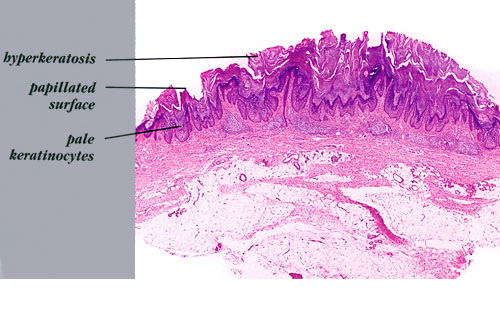
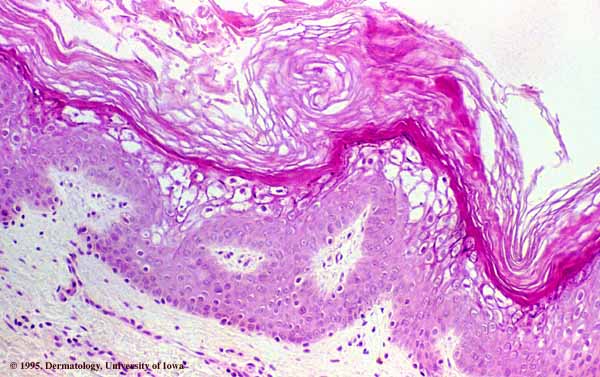
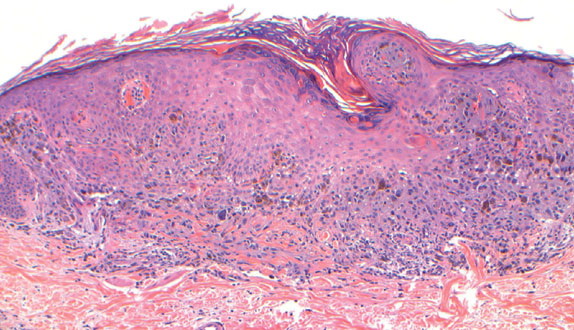
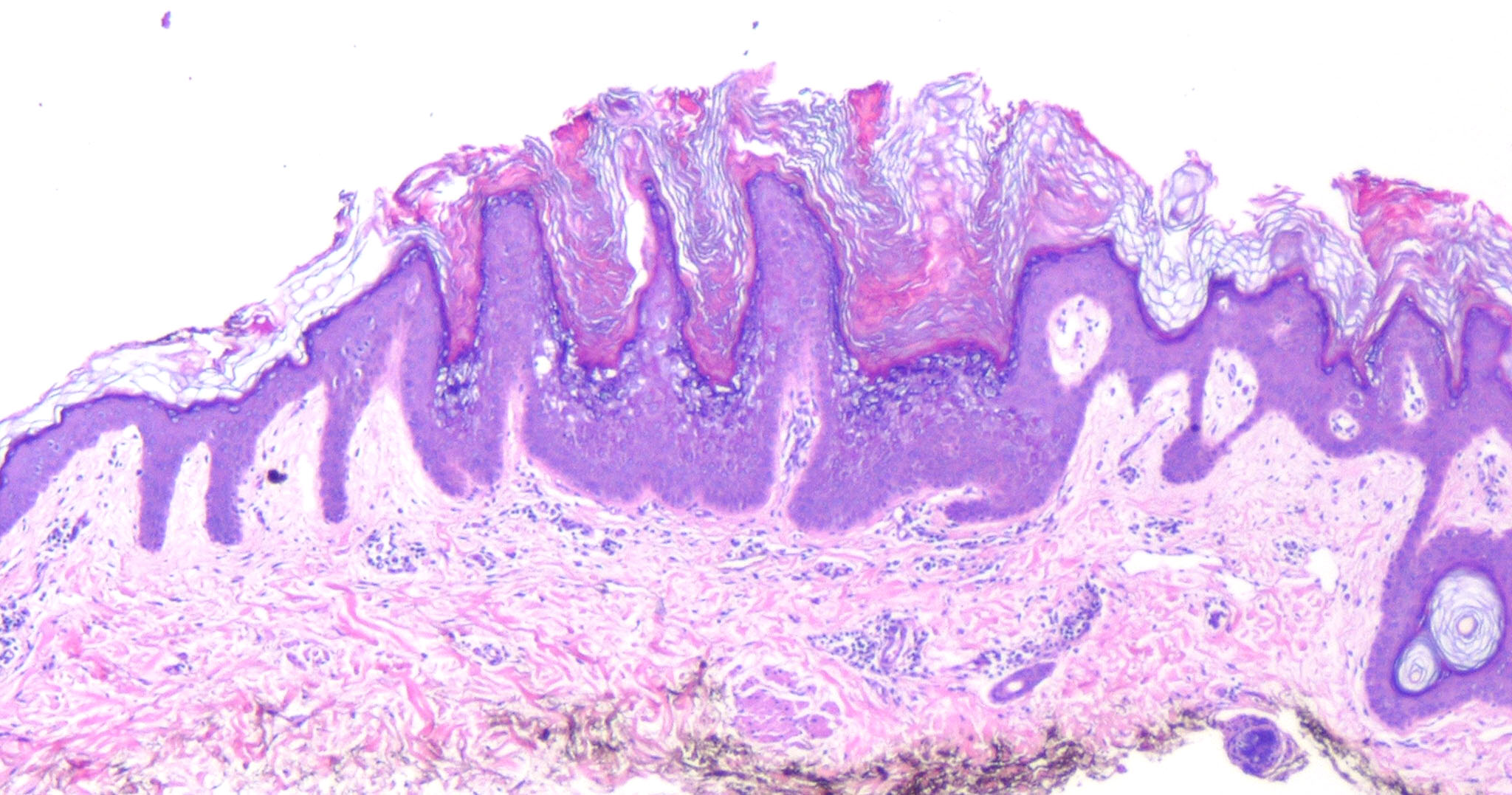
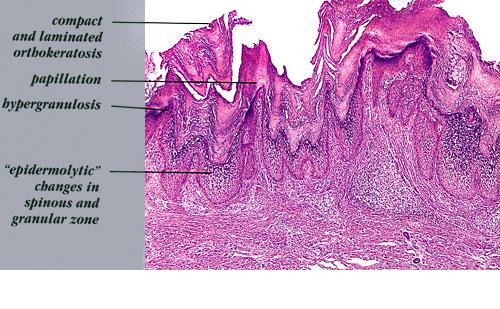
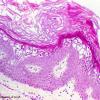
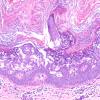
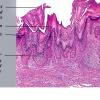
Histopathology. A characteristic histologic picture is seen in the epidermis and is referred to either as epidermolytic hyperkeratosis or as granular degeneration . It is present in bullous as well as in non bullous areas. There are variously sized clear spaces around the nuclei in the upper stratum spinosum and in the stratum granulosum. Peripheral to the clear spaces, the cells show indistinct boundaries formed by lightly staining material or by keratohyaline granules. A markedly thickened granular layer containing an increased number of irregularly shaped keratohyaline granules and compact hyperkeratosis is observed (14). When bullae form, they arise intraepidermally through separation of edematous cells from one another . The upper dermis shows a moderately severe, chronic inflammatory infiltrate. Mitotic figures are five times more numerous than in normal epidermis .
Pathogenesis.
Defects in keratin genes (KRT1 and KRT10) (16) are now known to be associated with this disorder. Mutations have been found in the carboxy terminal of the rod domain of keratin 1 and the aminoterminal of the rod domain of keratin 10 (17). The essential electron microscopic features are excessive production of tonofilaments and excessive and premature formation of keratohyaline granules; thus, at the periphery of the cells, numerous keratohyaline granules are embedded in thick shells of irregularly clumped tonofilaments (. The desmosomes appear normal, but the association of tonofilaments and desmosomes is disturbed, so many desmosomes are attached to only one keratinocyte instead of connecting two neighboring keratinocytes. Because of this disturbance in desmosomal attachment, blister formation takes place and real acantholysis occurs . Labeling with tritiated thymidine reveals greatly increased proliferative activity in the epidermis . It can be concluded that keratinization is both excessive and abnormal.
Differential Diagnosis. Although the histologic picture of epidermolytic hyperkeratosis is diagnostic for the type of ichthyosis called epidermolytic hyperkeratosis, it is not specific for it. Hyperkeratosis is found also in several other seemingly unrelated conditions : epidermolytic keratosis palmaris et plantaris, solitary epidermolytic acanthoma, disseminated epidermolytic acanthoma, and linear epidermal nevus, usually of the systematized type. This latter entity was thought to be an entirely different condition than epidermolytic hyperkeratosis but with similar histologic findings. However, it is now known that epidermal nevi of the epidermolytic hyperkeratotic type are a mosaic genetic disorder of suprabasal keratin (l.e., point mutations of 10k alleles of epidermal cells in
keratinocytes from lesional skin) that can be transmitted to offspring producing generalized epidermolytic hyperkeratosis . Epidermolytic hyperkeratosis can be an incidental finding in a variety of conditions
|
|