|
Epidermolysis bullosa acquisita = انحلال البشرة الفقاعي المكتسب |
 |
 |
 |
|
Epidermolysis Bullosa Acquisita
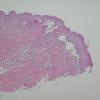
Classically, EBA is a noninherited disorder of acquired skin fragility. This presentation of EBA was the only one recognized until later. Blisters develop on noninflammatory bases with a predilection for acral areas. Scarring and milia formation ensue. A characteristic nail dystrophy and alopecia are noted. This presentation is associated with malignant lymphoma, amyloidosis, and colitis or enteritis. Some patients with EBA may have significant involvement of oral and conjunctival mucosa and therefore may be cicatricial pemphigoid-like. However, acral lesions are prominent and nail dystrophy may be noted In this type, biopsy from mucosal lesions reveals inflammatory, subepidermal bullae with scarring and milia similar to cicatricial pemphigoid.
|
|
In 1984, five EBA patients with clinical and histologic features of bullous pemphigoid were described (1 09). They had generalized pruritic, erythematous macules and papules on which bullae arose. There was less tendency for the lesions to develop acrally and greater involvement of flexural surfaces than in the previously described forms of
|
|
EBA. At presentation, neither scarring nor milia were discemed; however, delicate scars developed later at the sites of blister formation.
|
|
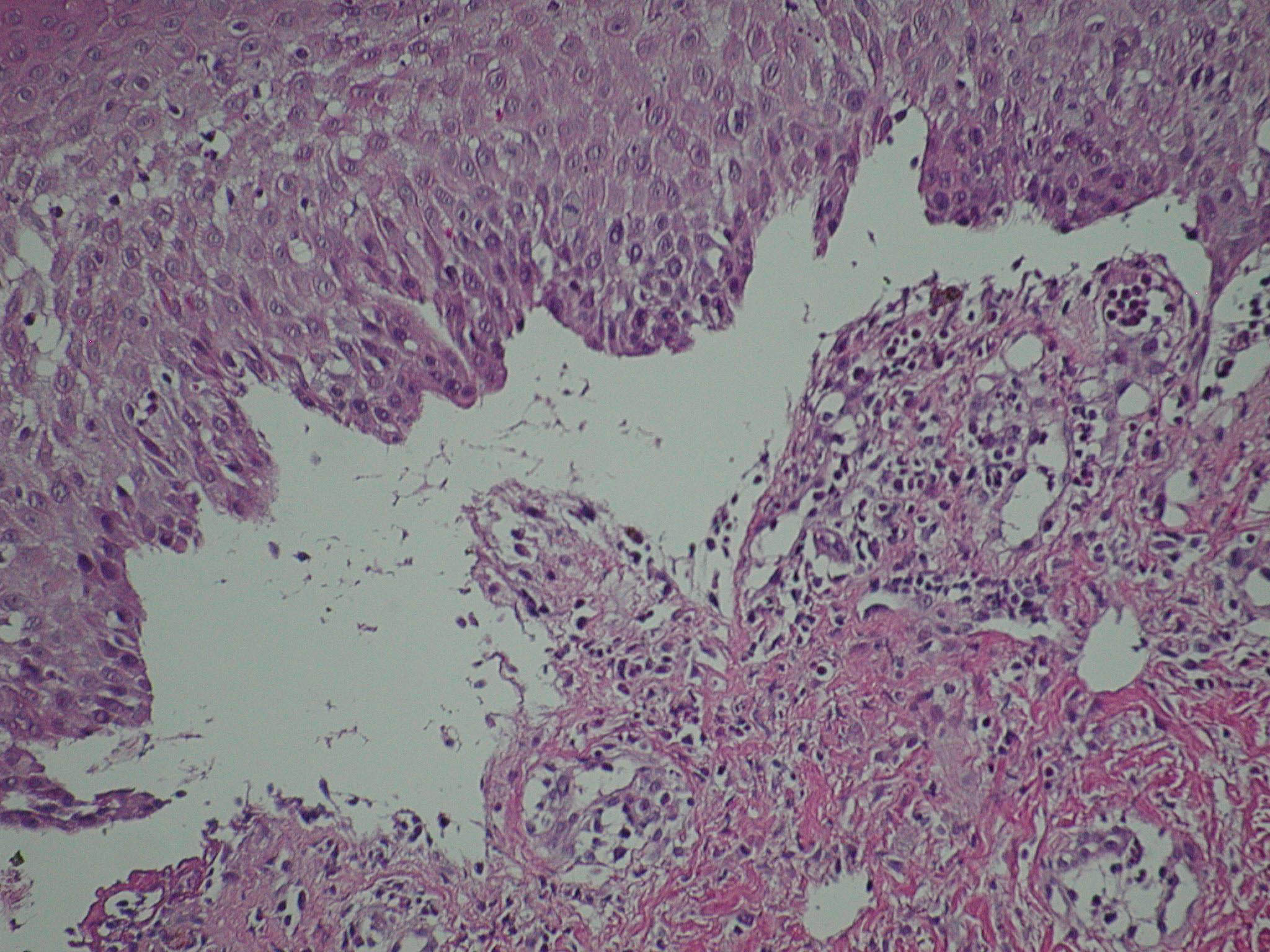
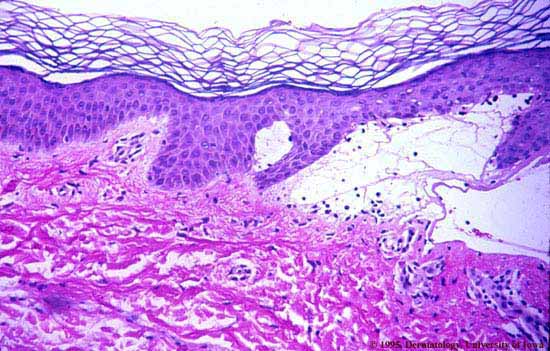
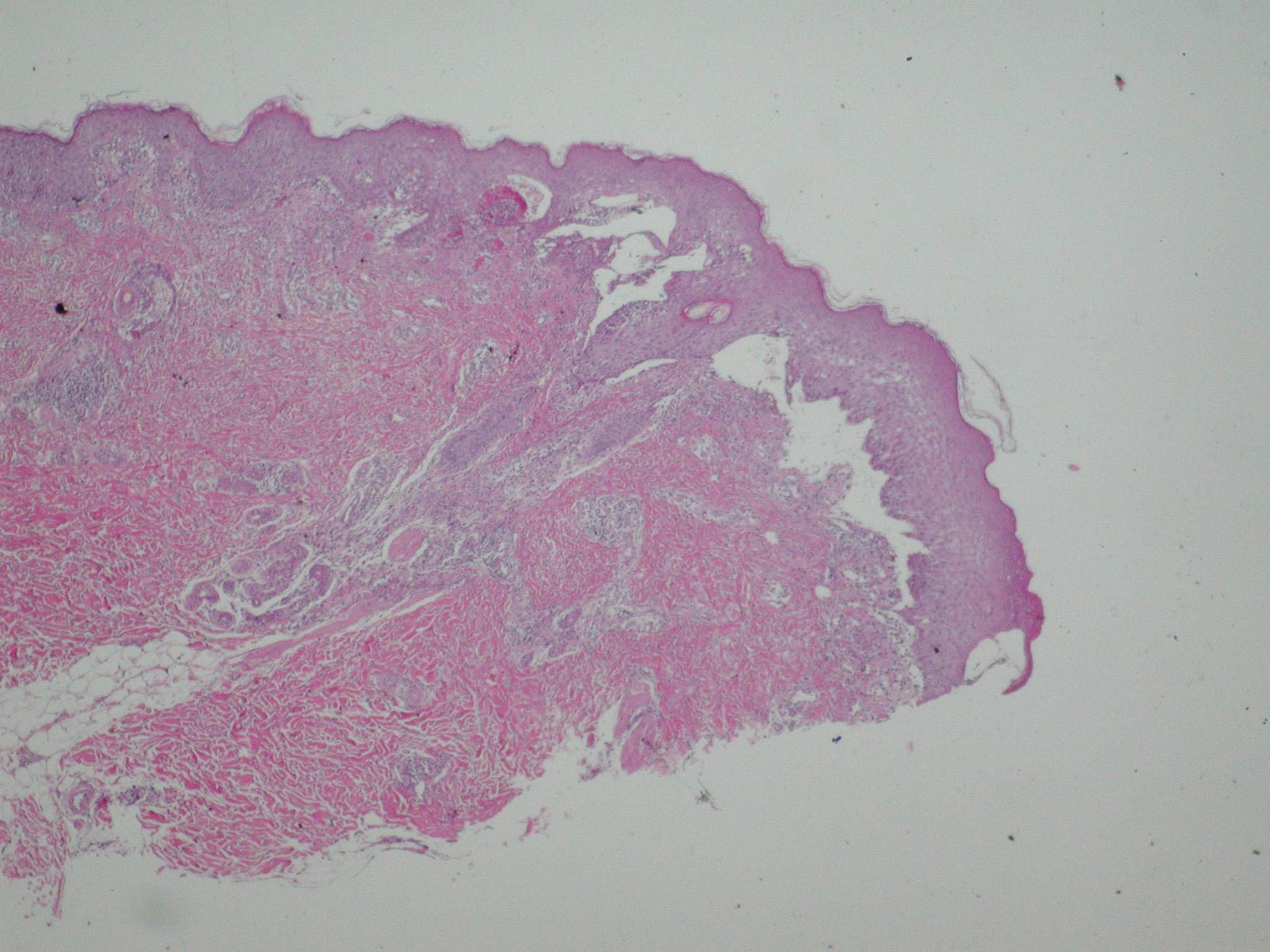
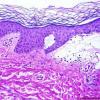
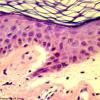
Histopathology.
The bullous pemphigoid-like presentation described above is the most common form of EBA. The subepidermal blisters are inflammatory. The predominant infiltrating cells are lymphocytes and neutrophils in perivascular and focal interstitial array. Eosinophils are present in variable numbers . In the classic form, the subepidermal blisters are noninflammatory ; fibrosis and milia formation are often present.
|
|
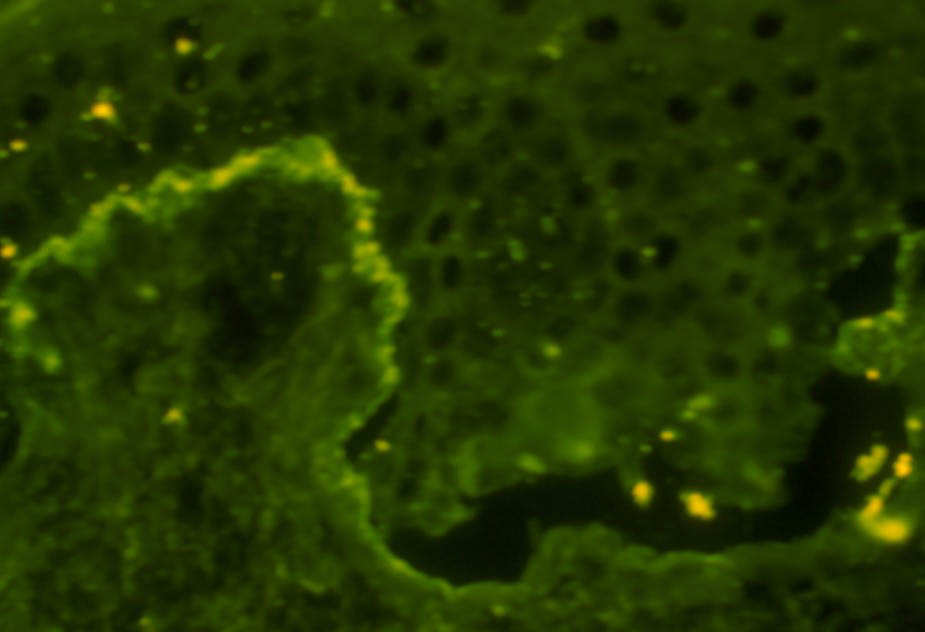
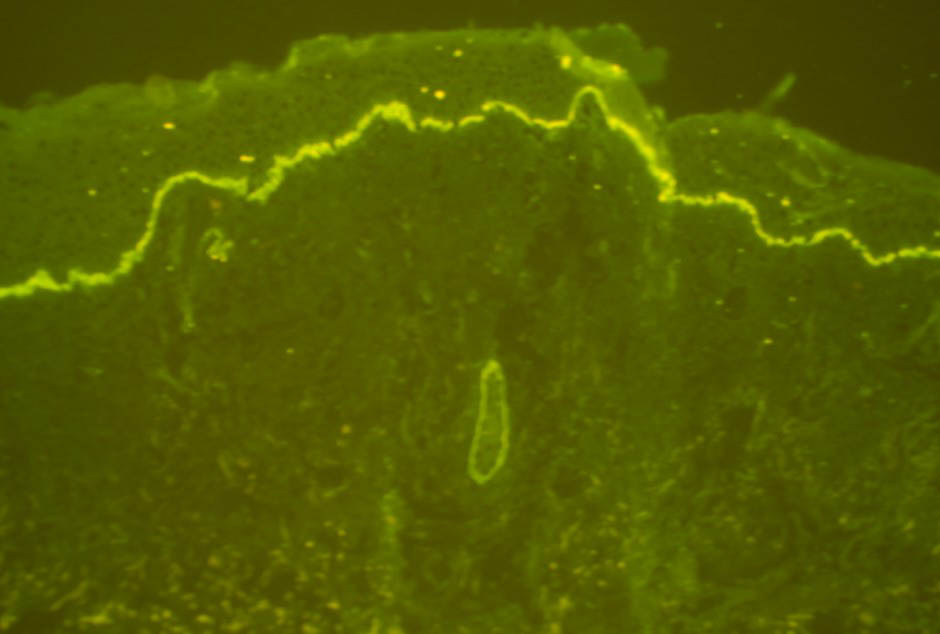
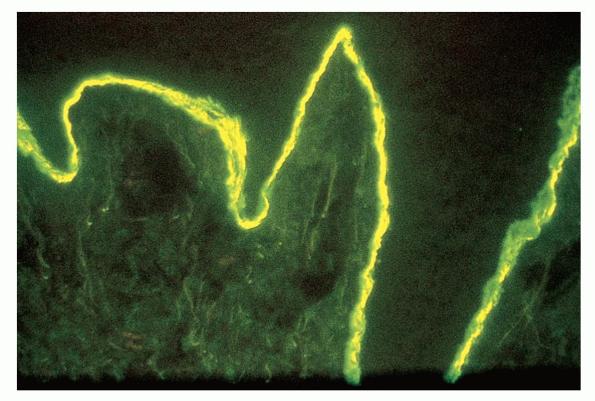
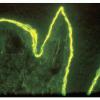
IF Testing.
Examination of perilesional skin using DIF reveals linear deposition of complement at the basement membrane zone in the vast majority of cases. IgG is by far the most common immunoglobulin found, but IgM and IgA may be present as well. Increasing numbers of immunoglobulin subclasses noted at the dermal-epidermal junction favor a diagnosis of EBA over bullous pemphigoid. The presence of linear C3 at the dermal-epidermal junction alone favors bullous pemphigoid over EBA. However, use of routine DIF cannot reliably distinguish between bullous pemphigoid and EBA. IIF reveals circulating anti-basement membrane zone antibodies in up to 50%.
|
|
The use of the salt-split skin technique leads to the appropriate diagnosis in most cases . The antibodies in EBA have specificity for the globular carboxyl terminus of type VII collagen and are deposited beneath the lamina densa. Therefore, on salt-split skin studies, IgG is on the floor and not on the roof of the split .
|
|