| Bacillary angiomatosis = الورام الوعائي العصوي |
|
|
BACILLARY
ANGIOMATOSIS
Epidemiology BA is most commonly seen in patients with acquired immunodeficiency syndrome (AIDS) and a CD4 count less than 50 cells/mm3, with an incidence of 1.2 cases per 1000 at-risk patients Patients with other forms of immunosuppression, including patients with leukemia and recipients of organ transplants, have been reported. Uncommonly, human immunodeficiency virus-negative and nonimmunosuppressed persons develop BA. In the cases of BA in immunocompetent persons, however, although the lesions were proliferative vascular papules, they were limited in number, the affected persons had limited or no systemic involvement and a benign course. There is no predisposition in terms of race, sex, or age. BACILLARY ANGIOMATOSIS AT
AGLANCE
Etiology and Pathogenesis Both B. henselae (the CSD bacillus) and B. quintana (the agent of trench fever) have been identified as causative agents of BA. At one end of the clinical spectrum, classic CSD is seen in young, immunocompetent hosts as a limited infection. At the other end, BA is seen in patients who are severely immunocompromised as a systemic disease. Thus, it is the immunocompetence of the host and the bacterial load that dictates the clinical manifestations of the disease. Moreover, immunocompromised patients with BA develop an angioproliferative response in response to intracellular hypoxia. The presence of intracellular bacilli induces hypoxia-inducible factor-1 that in turn induces vascular endothelial cell growth factor, leading to vascular proliferation.29 BA caused by B. henselae is acquired from infected cats and is a manifestation of CSD in the immunocompromised host. Peliosis hepatitis is exclusively associated with B. henselae infection.33 In contrast, patients with BA caused by B. quintana develop subcutaneous masses and lytic bone lesions. Clinical Manifestations CUTANEOUS LESIONS The incubation period for BA is unknown. In AIDS patients, the clinical constellation includes fever, cutaneous or subcutaneous vascular lesions, lymphadenopathy, and/or abdominal symptoms. The most common cutaneous morphologies of BA are (1) pyogenic granuloma-like lesions, (2) subcutaneous nodules, and (3) hyperpigmented indurated plaques. The same patient may have several morphologies. Lesions resembling pyogenic granuloma can range in size from 1 mm to many centimeters and are dusky-red in color with a collarette of scale and peripheral satellite lesions . The lesions are firm, bleed easily, and are often tender. They occur on skin and mucosa. Subcutaneous nodules can range from distinct nodules to diffuse swellings
Box 182-2 Differential Diagnosis of Bacillary Angiomatosis Most Likely
Consider
Always Rule Out
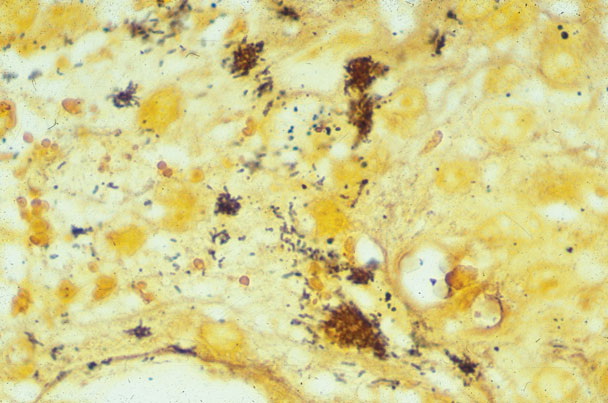
RELATED PHYSICAL FINDINGS In addition to cutaneous lesions, other organ systems may be affected. Hepatic and splenic vascular lesions can occur concomitantly with or independently of cutaneous lesions and can be a cause of significant blood loss and anemia. Bartonella infection, especially that caused by B. quintana, can affect bone and soft tissues. Lesions of the central nervous system have been reported and can result in neurologic and psychiatric disorders. Bacteremia, chronic fevers, and pulmonary and gastrointestinal lesions have also been reported. Radiologic studies usually identify areas of systemic involvement. Ocular vascular proliferative lesions can produce loss of vision.34 There are several reports of patients with other cutaneous diseases concomitant with BA, as well as the simultaneous existence of BA and another infection within the same lesion. Several patients have been reported with both BA and Kaposi sarcoma. Cytomegalovirus, Epstein-Barr virus, Cryptococcus neoformans, and Mycobacterium avium-intracellulare have been found within lesions of BA. Differential Diagnosis Laboratory Findings Patients with AIDS and BA are anemic and may have elevated liver function tests (characteristically, lactic acid dehydrogenase and alkaline phosphatase are more elevated than hepatocellular enzymes). Blood cultures are positive for Bartonella sp. in approximately one-half of BA patients. B. henselae and B. quintana can be cultured from skin lesions. The organisms grow slowly and may not be detected without prolonged culture (more than 1 month). PCR of affected tissue is virtually always positive if lesions are histologically characteristic. The vast majority of cases are diagnosed histologically, with identification of the causative bacteria by Warthin-Starry staining. Histopathology
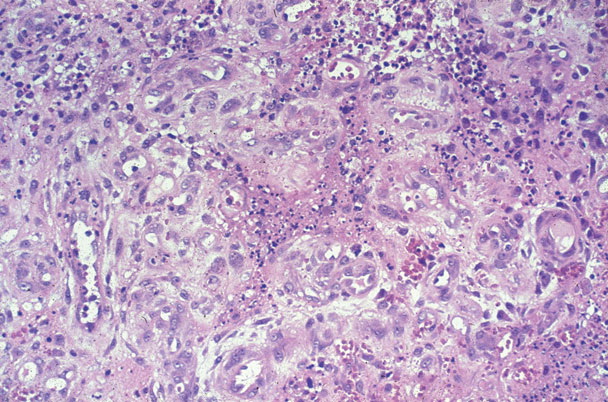
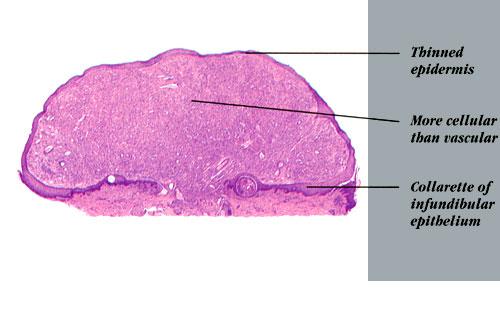
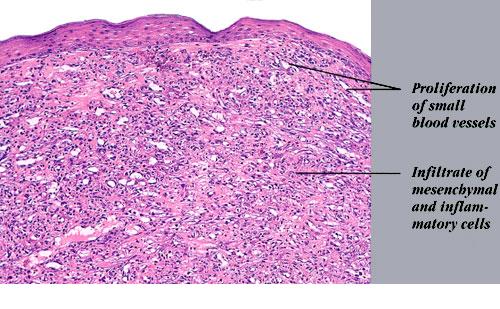
Lesions of BA have the general features of a lobular capillary hemangioma (pyogenic granuloma) , but in contrast to a pyogenic granuloma, the endothelial cells are often larger and polygonal; they may have marked atypia. There is a prominent inflammatory
Clinical Course In the immunocompromised host, the natural history of untreated BA is gradually progressive disease, with increasing numbers of skin lesions and involvement of many visceral organs. Untreated, severely immunocompromised patients might die of their infection. Treatment Erythromycin, 500 mg four times a day, or doxycycline, 100 mg twice a day for 3 months, is the treatment of choice for BA. Other antibiotics thought to be effective are minocycline, tetracycline, chloramphenicol, azithromycin, and roxithromycin. For peliosis hepatis, 4 months of treatment is recommended. Some patients require life-long suppressive therapy. Relapses have been reported, especially with shorter treatment courses. A Jarisch-Herxheimer reaction not uncommonly occurs after initiation of therapy. Most patients respond rapidly to antibiotic therapy. The rapid disappearance of the vascular lesions may relate to the effects of the macrolides and tetracyclines on protein synthesis, stopping the production of vascular growth factors. If patients are not treated for a sufficient period, they are likely to relapse, despite the fact that their skin lesions vanish after a few weeks of treatment. The additional treatment is required to sterilize visceral or hematologic reservoirs of bacteria. |