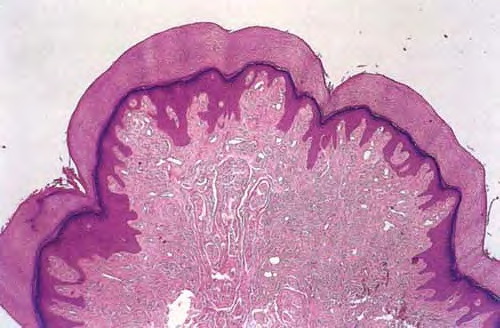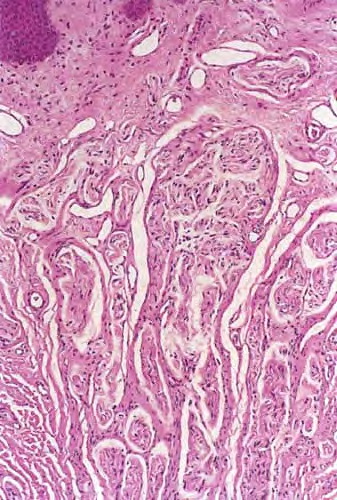
Supernumerary Digit
Polydactyly is the most common congenital digital anomaly of the hand and foot. It may appear in isolation or in association with other birth defects. Isolated polydactyly is often autosomal dominant or occasionally random, while syndromic polydactyly is commonly autosomal recessive.
Polydactyly should not be considered as a single mendelian trait but rather multifactorial. Early theories for polydactyly concerned disorders in the programmed cell death cycle of fetal limb development. Current theories focus on mutations in specific genetic locations that cause limb development to go awry. Mammals have been shown to have genetic clusters identified as homeobox or Hox genes corresponding to 5 domains across the limb bud. According to Muragaki et al, mutations in the HOXD13 gene are associated with synpolydactyly. As limb growth in utero progresses along a preset time line, elongation of the limb, development of soft tissue, and differentiation of digits progresses.
The Medscape Genomic Medicine Research Center may be of interest.
The epidemiologic data on postaxial polydactyly is limited because most birth defect registries do not include them, preferring to focus on defects linked to teratogens. Despite being a common malformation, the true incidence of polydactyly is not fully known.
One study by Finley et al combined data from Jefferson County, Alabama and Uppsala County, Sweden. This study showed incidence of all types of polydactyly to be 2.3 per 1000 in white males, 0.6 per 1000 in white females, 13.5 per 1000 in black males, and 11.1 per 1000 in black females. The Swedish data alone showed polydactyly of all types to have an incidence of 1.0 per 1000, equally distributed between males and females.
While the incidence of preaxial and postaxial polydactylies has been investigated, central polydactyly has not been fully studied.
Genetic and ethnic factors greatly influence the nature of polydactyly in the world population. Unfortunately, the knowledge of polydactyly is limited to select studies of certain subpopulations. Preaxial polydactyly is very common in various Asian populations, accounting for 90% of cases in South China, Hong Kong, and Japan. Duplicated thumbs at the metacarpophalangeal level are the usual anomaly.
Postaxial hand polydactyly is a common isolated disorder in African black and African American children, and autosomal dominant transmission is suspected. Postaxial polydactyly is approximately 10 times more frequent in blacks than in whites and is more frequent in male children. In contrast, postaxial polydactyly seen in white children is usually syndromic and associated with an autosomal recessive transmission.
Other factors associated with postaxial hand polydactyly include male sex, twinning, low maternal education, parental consanguinity, and recurrence in first-degree relatives. Postaxial polydactyly is associated with Amerindian, parental subfertility, and bleeding in the first trimester.
Polydactyly is the most common congenital digital anomaly of the hand and foot. It may appear in isolation or in association with other birth defects.
- Temtamy and McKusick6 classified polydactyly into preaxial, central, and postaxial types.
- Preaxial polydactyly, the most common type, refers to the duplication of the first digit or ray.
- Central polydactyly involves duplication of the second, third, or fourth digit or ray.
- Postaxial polydactyly involves the fifth digit or ray. The terms radial, central, and ulnar have been proposed more recently as an alternative subclassification to describe polydactyly in the upper extremity.
- Similarly, the terms tibial, central, and fibular have been proposed to describe polydactyly in the lower extremity. Initially, polydactyly in the foot was believed to be a variant of the hand. Yet, findings show the association of hand and foot polydactyly to be uncommon.
- Even more rare is crossed polydactyly, where preaxial involvement of one extremity is coupled with postaxial involvement of the opposite end of the body.
- Synpolydactyly is the combination of syndactyly and polydactyly.7
Treatment
Surgical management depends greatly on the complexity of the deformity. Postaxial polydactyly of the foot most commonly is treated with surgical removal for cosmesis and shoe comfort. Waiting until age 9-12 months is advisable to decrease anesthesia risk. A related eMedicine article is Polydactyly of the Foot.
A child with distal extremity anomalies experiences emotional stress. By age 3 years, the child has become aware of the anomaly. By age 7 years, the child has begun to experience the close scrutiny of his peers at school. For these reasons, as well as others, surgical correction should be initiated early in life. Needless to say, psychological support should be provided for patients and parents facing these challenges.