| Granuloma inguinale = الورم الحبيبي الاربي |
|
|
Granuloma Inguinale
▪ EPIDEMIOLOGY AND MODE OF TRANSMISSION
The mode of transmission of granuloma inguinale (GI) is controversial. It is generally considered sexually transmitted, but fecal contamination and autoinoculation remain a possibility, especially in the setting of infected children and adults without sexual activity and primary involvement of remote extragenital sites. Transmission rate between sexual partners is low compared with other sexually transmitted diseases and was found to be not more than 50 percent. The incidence of GI is also relatively low among both prostitutes and their conjugal partners. Nevertheless, this disease predominantly affects sexually active individuals. Moreover, donovanosis, being an ulcerative disease, increases the risk of human immunodeficiency virus (HIV) transmission. Transvaginal transmission of donovanosis during delivery has been reported, with an apparent predilection to ear structures of the newborn.7,8 Patients tend to belong to the low socioeconomic classes. No racial predilection has been proved, and both male and female predominance have been reported. Afflicted people are likely to delay seeking medical attention due to the painless nature of the ulcers and the possible embarrassment or fear from medical or surgical intervention. Late cases can be very debilitating and are much more difficult to manage. GI is endemic in warm, moderately humid areas like South Africa, India, Southern China, and Brazil.5,13 There are new endemic areas of donovanosis, mainly South and Central America, India, and Papua New Guinea,12 but the overall incidence of GI seems to be decreasing, especially in Papua New Guinea.1 The disease has nearly been eradicated from Australia, with only five cases reported in 2004, and is rare in North America and Europe.
▪ ETIOLOGY
Donovanosis is caused by the organism Klebsiella granulomatis, previously called Calymmatobacterium granulomatis. The name has been changed after sequencing the phoE and 16S ribosomal RNA genes and demonstrating close homology with K. pneumoniae and K. rhinoscleromatis. K. granulomatis is a Gram-negative, nonmotile, pleomorphic bacterium that stains well with Giemsa, Wright's, or silver stains but is periodic acid-Schiffnegative. The mature form is encapsulated, while the immature form is not. The immature non-encapsulated form may assume a closed-safety-pin appearance due to bipolar chromatin densities. It is difficult to culture and store this organism; however, it may be cultured using embryonic chick heart or chick embryo amniotic fluid. It has also been cultured in human peripheral blood mononuclear cells after decontaminating the specimen with amikacin, vancomycin, and metronidazole, and in HEp-2 cells after adding gentamicin and cycloheximide.
GRANULOMA INGUINALE AT AGLANCE
K. granulomatis is a facultative organism that resides in the cytoplasm of large mononuclear cells. It is pathogenic only to humans and the developing chick embryo. It was isolated from the feces of two out of four patients with donovanosis, although it has not been successfully cultured from feces. It is still unknown if this organism has a natural habitat.18
▪ CLINICAL FINDINGS: HISTORY AND CUTANEOUS LESIONS
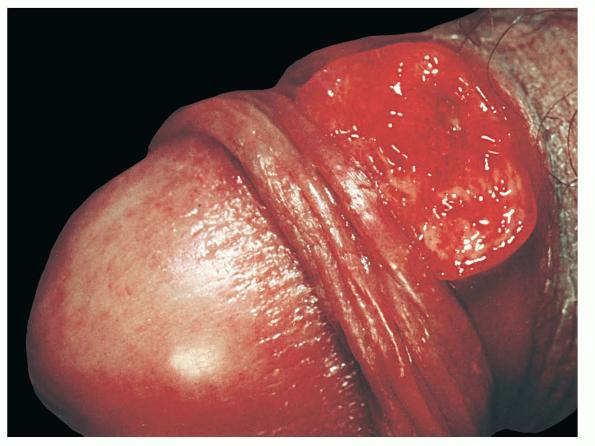
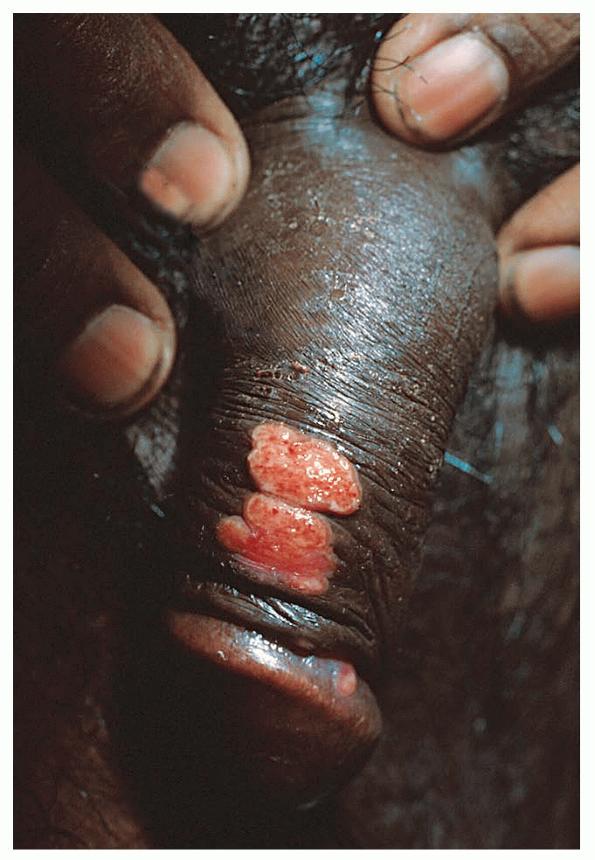
The incubation period extends from 3 days to 3 months but is usually 2 to 3 weeks. Single or multiple papules or nodules later develop and grow into a painless ulcer that may extend to the adjacent tissues and moist folds, forming “kissing lesions.” The penis, scrotum, and glans are the most commonly affected sites in males; and the labia and perineum are most commonly affected in females.11 Vaginal and cervical involvement has also been reported and sometimes mistaken for squamous cell carcinoma. The anus and colon may be infected, especially in homosexual males. GI most commonly presents as beefy red, easily bleeding, foul-smelling ulcers with granulation tissue. The ulcers may have hypertrophic or verrucous borders resembling condylomata acuminata. It may also present as soft, red nodules that eventually ulcerate . In long-standing donovanosis, the lesions may be necrotic, quite destructive of tissue, and have a copious gray, foul-smelling exudate. The tissue overlying the regional lymph nodes may evolve into an abscess or pseudobubo that later ulcerates. The lymph nodes per se are rarely involved unless there is a bacterial superinfection. In the rare dry cicatricial form, the nonbleeding ulcers form band-like scars and lead to digital lymphedema due to constriction. HIV co-infection may alter the clinical presentation of GI. The natural history is usually more rapid, and ulcers may persist for longer periods, lead to more tissue destruction, and need more prolonged antibiotic treatment. Extragenital dissemination of GI has been reported in HIV-positive patients.
▪ DIAGNOSIS AND LABORATORY TESTS
Demonstrating the Donovan bodies on smear or biopsy specimen makes the diagnosis of GI, although they are more easily visualized with properly done smears rather than biopsy. Secondary bacterial infection and debris may affect the smear result; thus it is recommended to wipe the ulcers gently with cotton swabs first before taking the smear but not to clean the ulcers with saline first. Tissue for smear or crush preparations are better taken from the advancing edge of the ulcer, and tissue preparation should be made immediately, before the desiccation of histiocytes. Serology is not helpful in making the diagnosis. Polymerase chain reaction has so far only been used for research purposes. Histologically, the epidermis may exhibit pseudoepitheliomatous hyperplasia and/or ulcerations, depending on the site biopsied. In the dermis, a dense mixed inflammatory cell infiltrate is usually seen composed of polymorphonuclear cells, plasma cells, histiocytes, and rare lymphocytes. Edema and endothelial cell swelling are often noted. The hypertrophic and the cicatricial forms of GI may exhibit fibrosis. Clusters of Donovan bodies are seen in the vacuolated cytoplasm of the large mononuclear cells. Using Giemsa, Wright's, or silver stains, these Donovan bodies appear as safety-pin-like structures measuring 1 to 2 µm × 0.5 to 0.7 µm. These Donovan bodies may also be occasionally found extracellularly or within neutrophils. Box 204-1 Differential Diagnosis of Granuloma Inguinale Most Likely
Always Rule Out
The differential diagnosis of Donovan bodies includes the Frisch bacilli in Mikulicz cells of rhinoscleroma, the amastigotes of leishmania, the chlamydial inclusion bodies of lymphogranuloma venereum, histoplasmosis, and the Michaelis-Gutmann bodies of Malakoplakia.
▪ COMPLICATIONS
Genital complications of donovanosis include genital swelling that may progress to pseudoelephantiasis, phimosis, paraphimosis, and progressive tissue destruction that may lead to the destruction of the whole penis or other involved organs. There is also an increased risk of squamous cell carcinoma in long-standing cases. Extragenital involvement has been reported in around 6 percent of the cases, occurring either as a primary infection or by spreading from a genital site by autoinoculation or systemic hematogenous dissemination. Primary extragenital sites reported include particularly the oral mucosa, and also the neck, scalp, chest, arms, and legs. Oral involvement usually presents as swelling, ulcerations, and bleeding of the gum and palate. Bone involvement may lead to loss of teeth. Long-standing infection results in fibrosis, gum and cheek adhesions, and microstomia.5,6 Hematogenous dissemination may present with fever, anorexia, and weight loss. It may lead to the involvement of bones, notably, and other visceral organs like the abdominal cavity, bowel, liver, spleen, and lungs. The most commonly affected bone is the tibia, comprising more than 50 percent of reported cases. There are few reported cases of GI manifesting as otitis media with mastoiditis, psoas abscess, and cervical lymphadenopathy. In addition, the fact that GI ulcers are painless and bleed easily upon contact increases the risk of HIV transmission remarkably. ▪ PROGNOSIS AND CLINICAL COURSE GI shows no tendency for spontaneous healing. If left untreated, GI may extend to internal organs, including the ovaries, adnexa, uterus, epididymis, and bladder. Fistulas may form and lead to genital fibrosis and deformity.5,11 Systemic dissemination may be fatal, especially in cases of misdiagnosis.6
▪ TREATMENT
Untreated ulcers do not resolve spontaneously. On the contrary, they tend to worsen with time, and antibiotic treatment is better started early . The patient should continue treatment until all clinically visible ulcers have completely healed. Serial biopsy specimens may be needed. If the patient does not improve within the first few days of treatment, the addition of gentamicin 1 mg/kg intravenously every 8 hours needs to be considered. The Centers for Disease Control and Prevention recommends the same treatment regimens for HIV-positive patients with GI, although there have been few reports of failure of such treatment. The Centers for Disease Control and Prevention also strongly recommends gentamicin 1 mg/kg intravenously every
Treatment of Granuloma Inguinale
Relapse may occur 8 to 16 months after apparently effective treatment, requiring follow-up by the physician. Long-standing cases may be complicated by secondary bacterial infections or by fistulas and abscess formation, which require surgical intervention and render antibiotic treatment alone ineffective.13 Pregnant or lactating patients with GI are to avoid doxycycline and ciprofloxacin in their treatment regimens.
▪ PREVENTION
All partners who had sexual contact with a patient with GI within 60 days before the onset of symptoms need to be examined. Sexual partners need not be treated unless they develop signs and symptoms of GI. Children born to mothers with untreated donovanosis need to receive prophylactic azithromycin at a dose of 20 mg/kg for 3 days.
|