| Gonorrhea = السيلان البني |
|
|
Gonorrhea and Other
Venereal Diseases
▪ GONORRHEA
Epidemiology
More than 700,000 people are reported to acquire new gonorrheal infections in the United States every year. Yet, only one-half of these infections are reported to the Centers for Disease Control and Prevention (CDC). The rate of new infections declined after the implementation of a national gonorrhea control program in the United States during the mid-1970s and has continued to decrease slightly since 1999. The prevalence of infection may have decreased due to screening programs that have incorporated immediate, on-site, single-dose treatment, if needed. Safer sex practices in response to the human immunodeficiency virus (HIV) epidemic may also be a contributing factor to the decline of new gonorrheal infections. The highest rate of reported gonorrheal infections is among sexually active teenagers, young adults, and African Americans. Such racial disparity is multifactorial and may be due to differences in accessibility to health care, lack of use of resources available, crowded living environments, and sexual partner preferences. Risk factors for acquisition of new gonorrheal infection include new or multiple sex partners, young age, unmarried status, minority ethnicity, substance abuse, lower socioeconomic and educational levels, and previous infection. Overall, since the 1980s, prevalence rates among men and women have been similar. The highest rates in women are for those between the ages of 15 and 19 years old and in men between the ages of 20 and 24 years old. A higher rate of new infections among men having sex with men has been reported recently in some major cities. Etiology and Pathogenesis Albert Ludwig Sigismund Neisser first discovered the causative agent of gonorrhea in 1879. Gonorrhea is caused by infection with Neisseria gonorrhoeae, a Gram-negative, aerobic coccus-shaped bacterium found in pairs. The organisms are usually visualized intracellularly in polymorphonuclear leukocytes . Gonorrhea is acquired through sexual contact, or, less commonly, as a result of poor hygiene or medical use of urine. It can also be transmitted vertically from mother to child during birth. Pathogenesis involves attachment to columnar epithelial cells via pili or fimbriae. The most common sites of attachment include the mucosal cells of the male and female urogenital tracts. Outer membrane proteins, PilC and Opa, on the bacteria aid in attachment and local invasion. Invasion is mediated by adhesins and sphingomyelinase, which contribute to the process of endocytosis. Certain gonococcal strains produce immunoglobulin A proteases that cleave the heavy chain of the human immunoglobin and block the host's bactericidal immune response. Once inside the cell, the organism undergoes replication and can grow in both aerobic and anaerobic environments. After cell invasion, the organism replicates and proliferates locally, inducing an inflammatory response. Outside the cell, the bacteria are susceptible to
GONORRHEA AND OTHER VENEREAL DISEASES AT A GLANCE
Clinical Findings: History and Physical Findings N. gonorrhoeae infection tends to involve mucous membranes consisting of columnar epithelial cells. The urethra, cervix, rectum, pharynx, and conjunctiva are the areas most commonly involved.
LOCALIZED DISEASE (MEN)
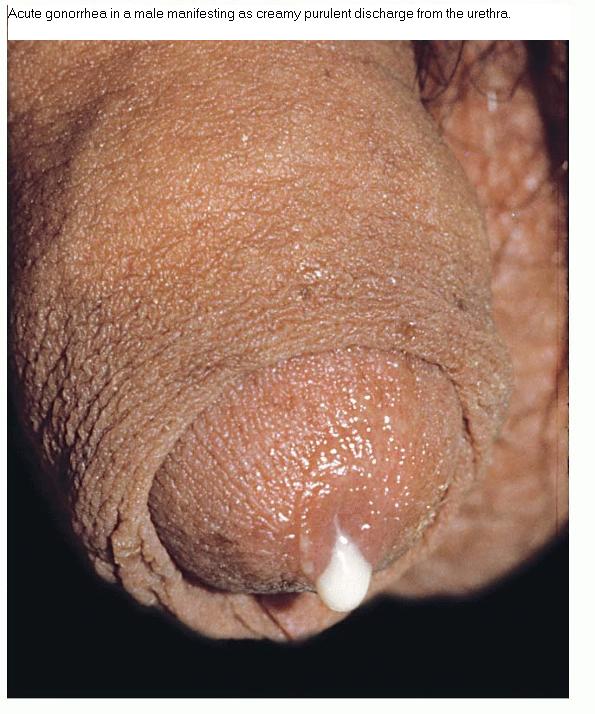
The incubation period for the bacteria in men ranges from 2 to 8 days, with most infections being symptomatic after 2 weeks. Only about 10 percent of infections are asymptomatic in men. The most common manifestation of gonococcal infection in men is urethritis, characterized by cloudy or purulent discharge from the penile meatus, which may be indistinguishable from other non-gonococcal causes . Mucosal membrane inflammation in the anterior urethra leads to painful urination and surrounding redness and swelling . Testicular pain and swelling may indicate epididymitis or orchitis and may be the only presenting symptom. However, epididymitis is more commonly caused by Chlamydia trachomatis or by combined infection with N. gonorrhoeae. Proctitis is another manifestation of gonococcal infection with symptoms including rectal mucopurulent discharge, pain on defecation, constipation, and tenesmus. Proctitis usually occurs in individuals who engage in anoreceptive intercourse and more commonly in men who have sex with men. As a result of gonococcal proctitis, men who have sex with men are at a higher risk of acquiring HIV infection due to damaged epithelial integrity. Pharyngitis caused by N. gonorrhoeae is rare and usually asymptomatic, although it may serve as a source for disseminated disease. Symptoms range from cervical lymphadenopathy and pharyngeal erythema to severe ulceration with pseudomembrane formation.
LOCALIZED DISEASE (WOMEN)
Fifty percent of women infected with N. gonorrhoeae are asymptomatic. Appropriate screening, prompt diagnosis, and treatment is crucial in women due to serious complications that can result in sterility. The endocervix is a common site of local infection and invasion by organisms. Symptoms of urethritis include mucopurulent discharge, vaginal pruritus, and dysuria. However, vaginitis does not occur except in prepuberal girls or post-menopausal women because the vaginal epithelium of sexually mature women does not support growth of N.
PID occurs in about 10 percent to 40 percent of uncomplicated gonorrheal infections in women and is characterized by fever, lower abdominal pain, back pain, vomiting, vaginal bleeding, dyspareunia, and adnexal or cervical motion tenderness on physical examination. Sequelae of untreated infection include tubo-ovarian abscesses, subsequent ectopic pregnancies, chronic pelvic pain, and infertility due to chronic inflammation with resultant scarring. Symptoms tend to occur at the time of menses and cannot be distinguished from non-gonococcal etiologies. Fitz-Hugh-Curtis syndrome, involving inflammation of the liver capsule, is associated with genitourinary tract infection and may be present in up to one-fourth of women with PID caused by either N. gonorrhoeae or C. trachomatis. Presenting symptoms include right upper quadrant pain and tenderness with abnormal liver function tests. Women may also develop proctitis through autoinoculation from cervical discharge or as a result of direct contact from an infected partner's penile secretions. Symptoms may include rectal mucopurulent discharge, pain on defecation, constipation, and tenesmus. The incidence of gonococcal pharyngitis is similar to that in men.
NEWBORNS AND CHILDREN
Neonates may acquire N. gonorrhoeae during passage through the birth canal from contact with infected secretions. Such ocular infections are known as ophthalmia neonatorum and can lead to severe corneal perforation or scarring. Most states, by law, require the prophylactic use of silver nitrate drops, erythromycin, or tetracycline ophthalmic ointment for prevention of ophthalmia neonatorum. Pharyngeal or genital gonococcal infection in children is often a sign of sexual abuse and warrants further investigation.
DISSEMINATED DISEASE
Spread of infection from the site of inoculation to other parts of the body through the bloodstream leads to disseminated gonococcal infection (DGI). Disseminated disease occurs in 0.5 percent to 3 percent of cases and is associated with the classic triad of dermatitis, migratory polyarthritis, and tenosynovitis. Pain and swelling may occur in a single joint or in multiple joints asymmetrically, with upper extremity joints affected more commonly than lower extremities. Skin findings consist of small macules or hemorrhagic pustules on an erythematous base located on palms and soles or on the trunk and elsewhere on the extremities . Skin lesions may develop necrotic centers; occasionally lesions may be similar in appearance to erythema nodosum or erythema multiforme. On the palms and soles, lesions may be tender, but in other sites they tend to be non-pruritic and painless and disappear after initiating appropriate treatment. Skin lesions may be present in 40 percent to 70 percent of cases of disseminated disease. Primary skin lesions as a result of localized gonorrheal infection are rare. Histologically, perivascular neutrophilia, dermal vasculitis, and epidermal neutrophil infiltration may be seen.
Laboratory Tests
Bacterial culture has been the “gold standard” diagnostic test for years, although newer and more specific tests are now being used in many laboratories. Culturing N. gonorrhoeae requires media containing heme, nicotinamide adenine dinucleotide, yeast extract, carbon dioxide, and other supplements required for isolation. Culture can be performed on modified Thayer-Martin medium. Organisms are Gram-negative, intracellular diplococci visualized microscopically inside polymorphonuclear cells. In men, culture and Gram's stain are performed on secretions or urethral swabs . Endocervical and endourethral specimens for culture and Gram's stain have yielded more accurate results than testing vaginal secretions in women. Cultures on pharyngeal and rectal swabs may also be performed if infection is suspected in these areas. The U.S. Food and Drug Administration has approved certain chemiluminescent DNA probes that can be used on endocervical or urethral specimens for diagnosis of gonorrhea. However, distinguishing gonococcal from non-gonococcal infection may be difficult with DNA probes. Newer techniques include the use of nucleic acid amplification tests, such as polymerase chain reaction (PCR), transcription-mediated amplification, and strand displacement amplification on urine or urethral specimens. Overall, nucleic acid amplification tests are highly sensitive and specific and may be able to detect even the presence of one organism. In DGI, cultures should be done on blood, joint fluid, and skin lesions. Synovial fluid from affected joints must be analyzed for cell count, Gram's stain, and culture. Diagnosis should be based on clinical suspicion and pertinent findings because tests for DGI yield positive results only in a small number of cases. Differential Diagnosis
Complications
Permanent sequelae of gonococcal infection in women may be infertility as a result of untreated PID. Untreated DGI can lead to septic arthritis, resulting in permanent joint damage. Meningitis and endocarditis are rare manifestations of DGI. Additional symptoms may include fever, malaise, and perihepatitis (Fitz-Hugh-Curtis syndrome). Prognosis and Clinical Course Prognosis is excellent if infection is treated early with appropriate antibiotics. Previously treated gonococcal infection
Differential Diagnosis for All Venereal Diseases
Treatment
Ten percent to 30 percent of people with gonococcal infection are co-infected with Chlamydia. Thus, routine dual therapy with doxycycline and azithromycin has been recommended and shown to be cost effective. Dual therapy also decreases the development of antimicrobial resistance in bacteria. Box 205-2 shows CDC recommendations for uncomplicated cervical, urethral, pharyngeal, and rectal gonococcal infections. Due to the increased prevalence of antimicrobial resistance, quinolones should not be used for infections acquired in California, the Pacific islands, including Hawaii, or Asia. Patients with DGI may need to be hospitalized due to septic arthritis, meningitis, or endocarditis. The recommended regimen for DGI is ceftriaxone, 1 g intramuscularly (IM) or intravenously (IV) every 24 hours, continuing for 24 to 48 hours after improvement is noted. Treatment may then be switched to oral doses of the antibiotics listed in Box 205-2. Sexual partners should also receive appropriate treatment. Box 205-2 Treatment of Localized, Uncomplicated Gonococcal Infection
Disseminated gonococcal infection requires longer treatment periods as shown in Table 205-1. Treatment of gonococcal meningitis should consist of ceftriaxone, 1 to 2 g IV every 12 hours for 10 to 14 days, and of gonococcal infections in neonates as shown in Box 205-3.
Box 205-3 Treatment of Gonococcal Infection in Neonates
or
Gonococcal ophthalmia neonatorum should be treated with ceftriaxone, 25 to 50 mg/kg IV or IM, not to exceed 125 mg in a single dose. Contraindications Women who are pregnant should not be treated with tetracyclines or quinolones due to possible damage to the fetus. A cephalosporin or a single 2-gram dose of spectinomycin can be used for gonococcal infection, and erythromycin or amoxicillin for chlamydia.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||