








FROSTBITE
Frostbite occurs when tissue freezes after exposure to extremely cold air, liquids, or metals. The clinical effects of accidental injury that leads to the death of tissues are similar to those caused by cryosurgery. The components of tissue that may lead to damage when frozen are water, with formation of ice crystals at 0°C (32°F), and lipids such as fat globules or cell membrane constituents.
The rate of freezing determines the site of injury at the cellular level. Extracellular formation of ice occurs most commonly with slow freezing, whereas fast freezing tends to produce intracellular ice. The formation of ice crystals in the extracellular space alters the osmotic properties of the tissues and disturbs the flow of water and electrolytes across the cell membranes. Thawing may be as damaging as the freezing itself, and repeated freeze and thaw cycles, as may occur in accidental injury, compound the damage, making more water available, which rapidly leads to intracellular flooding. The rewarming rate is also important. In slow rewarming, ice crystals become larger and more destructive. Cells are also exposed to a high concentration of electrolytes for a longer period than with rapid rewarming.
As the body cools, there is a reflex constriction of the arteries and veins in the extremities. This results in increased venous pressure, decreased capillary perfusion, and sludging. Cooling also creates a leftward shift in the oxygen dissociation curve, and hemoglobin gives up its oxygen less readily. These two conditions result in hypoxia and damage to the capillaries and surrounding tissue. Oxygen tension is further decreased by thrombus formation in the microvasculature, which results in arteriovenous shunting. Arterial and arteriolar constriction, mediated by sympathetic outflow, initiates and probably maintains circulatory impairment. In addition, segmental vascular necrosis occurs in areas of erythrostasis, which suggests that ultimate damage may depend more on insufficient clearance of toxic substances than on initial vasoconstriction.
Cell types vary in their susceptibility to cold injury. Melanocytes are very sensitive to cold, and irreversible damage may occur at -4°C to -7°C (24.8°F to 19.4°F). This sensitivity explains the hypopigmentation that follows cryotherapy. In addition, it appears that black persons are more susceptible to frostbite than whites. Nerve axons are also easily damaged by cold, and nerve injury may occur with axonal degeneration of large myelinated fibers. Autonomic fibers are also affected, and this may account for the abnormal sweating and cold sensitivity that follow nonfreezing cold injury.31,32 Nerve sheaths are quite resistant to cold, as are bone and cartilage.23 Desolidification of lipids in adipose tissue and disruption of endothelial cells lining blood vessels and lymphatics, with secondary disturbances of permeability and blood flow, are other consequences of severe cold. In the overall assessment, there are marked similarities in the pathologic processes to those seen in thermal burns and in ischemia-perfusion injuries.
Three stages of cooling are recognized. The first is massive vasoconstriction, which causes a rapid fall in skin temperature. In a second step, the hunting reaction follows with a cyclic rise and fall in skin temperature. If cold exposure continues, the third stage of freezing occurs as the skin temperature falls to approach ambient temperature. The events that ensue in freezing and nonfreezing cold injuries are similar. .
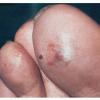
Frostbite usually affects a finger, toe, ear, nose, or cheek. The clinical presentation of frostbite falls into three categories
corresponding to mild frostbite or frostnip, superficial frostbite, and deep frostbite with tissue loss.














