| Erythema nodosum = الحمامى العقدة |
|
|
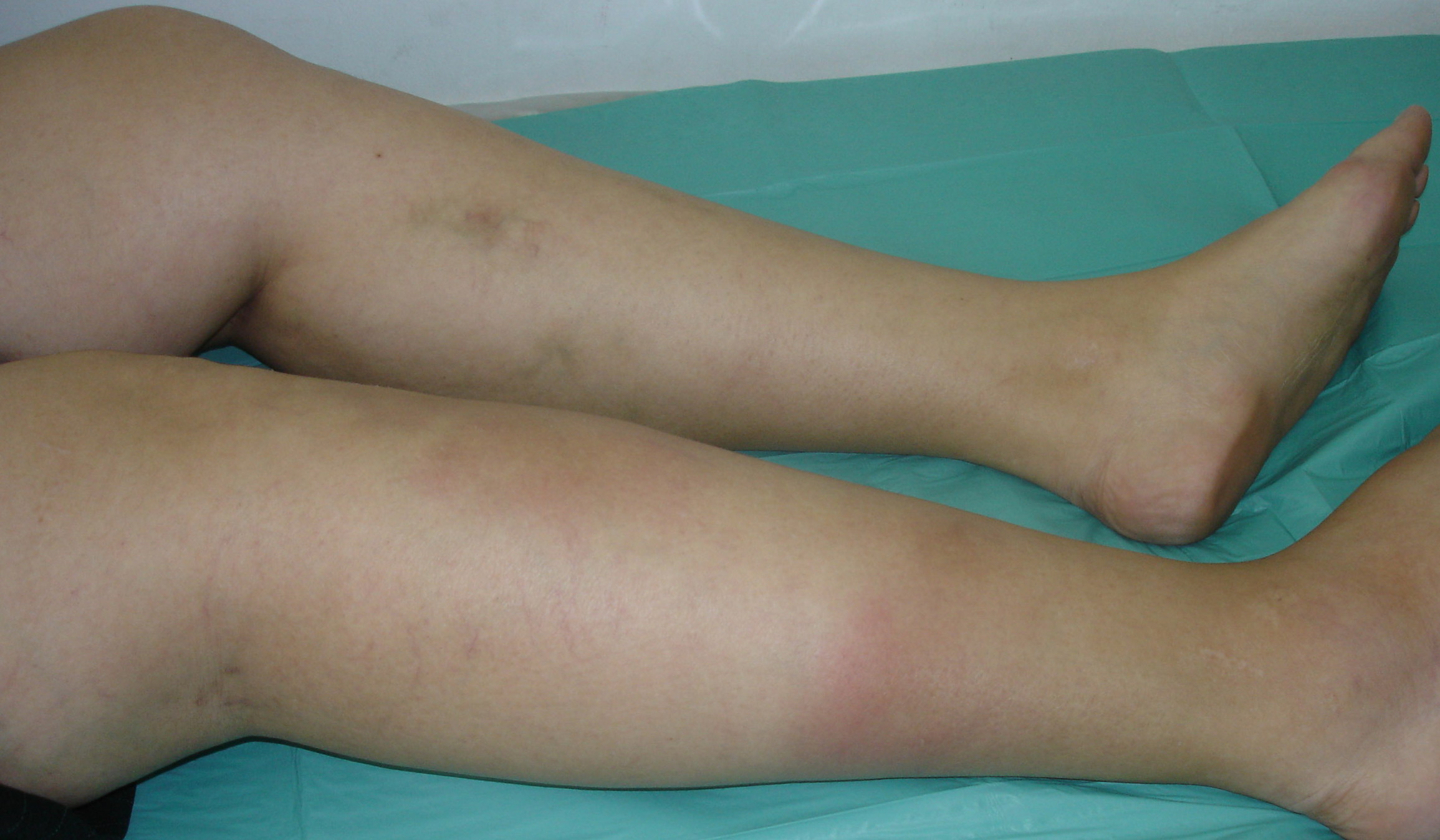
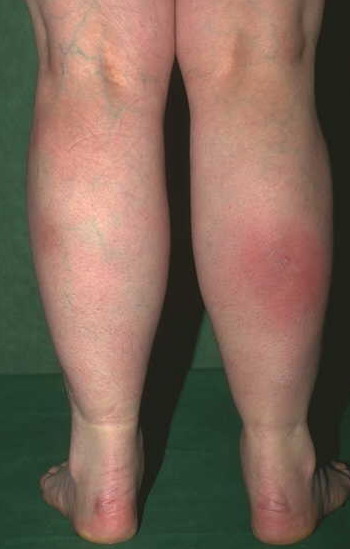
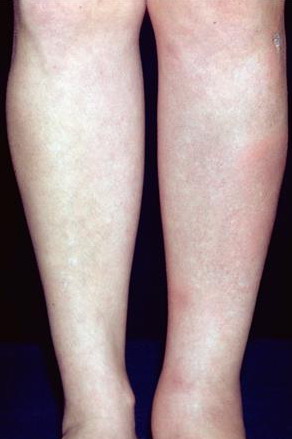
Erythema Nodosum Erythema nodosum is the most common type of septal panniculitis. It is not a disease but a reaction pattern to a variety
ERYTHEMA NODOSUM AT A GLANCE Clinical
Histopathology
Treatment
The classically described processes of erythema nodosum migrans,43-46 subacute nodular migratory panniculitis of Vilanova and Piñol, and chronic erythema nodosum,49 are now just considered clinical variants of erythema nodosum. The list of etiologic factors associated with erythema nodosum is very long, including infectious diseases, medications, malignancies, and a wide group of miscellaneous conditions (see Table 68-1).50-106 Although there are considerable geographic variations related to endemic infections, streptococcal infections are the most frequent etiologic factor of erythema nodosum in children. In contrast, drugs, sarcoidosis, and inflammatory bowel disease are the most commonly associated disorders in adults with erythema nodosum. Erythema nodosum is considered to be a hypersensitivity response to a large number of inciting factors. Erythema nodosum is the stereotypical histologic example of a mostly septal panniculitis with no vasculitis. The connective tissue septa of the subcutis appear thickened with inflammatory cells that extend to the periseptal areas of the fat lobules . As in other panniculitides, the composition of the inflammatory infiltrate in the septa of erythema nodosum lesions varies with age of the lesion, with neutrophils being the predominant cells in early lesions, whereas histiocytes and small granulomas are seen in late-stage lesions. A characteristic histopathologic marker of erythema nodosum is the so-called Miescher radial granuloma, which consists of small, round, well-defined nodular aggregations of small histiocytes radially arranged around a minute slit The nature of the central cleft is unknown, and immunohistochemical and ultrastructural studies have failed to demonstrate endothelial or other cellular lining of these clefts. In older nodules of erythema nodosum, histiocytes coalesce to form multinucleated giant cells , many of which still keep in their cytoplasm a stellate central cleft reminiscent of those centers of Miescher radial granuloma. Another histopathologic characteristic of erythema nodosum is the absence of vasculitis.110 In late-stage lesions of erythema nodosum, the septa are markedly widened with granulation tissue at the interface between septa and fat lobules. With time, the lesions resolve without atrophy or scarring of the involved septa. Treatment of erythema nodosum should be directed toward the associated disorder. Usually, nodules of erythema nodosum regress spontaneously within a few weeks, and bed rest is often sufficient treatment. Aspirin, nonsteroidal anti-inflammatory drugs and 2 to 10 drops of a saturated solution of potassium iodide may be helpful to enhance analgesia and resolution.111-116 Systemic corticosteroids are rarely indicated in erythema nodosum, and an underlying infection should be ruled out before these drugs are administered.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||