| Disseminated varicella zoster infection = انتان منتشر بفيروس داء المنطقة |
|
|
Disseminated varicella zoster infection Reactivation of varicella-zoster virus (VZV), also known as shingles, is a common health concern among patients aged 50 years or older and those with compromised immunity (Stankus, Dlugopolski, & Packer, 2000; Yawn et al., 2007) (see Figure 1). Reactivation of VZV is caused primarily by diminished cellular-mediated immunity from age-related immunosenescence, infections, and immunosuppressive agents (Burke et al., 1982; Yawn et al.). Disseminated VZV prevalence is relatively low, but VZV has been reported in patients following solid organ and stem cell transplantation and in patients receiving chemotherapy
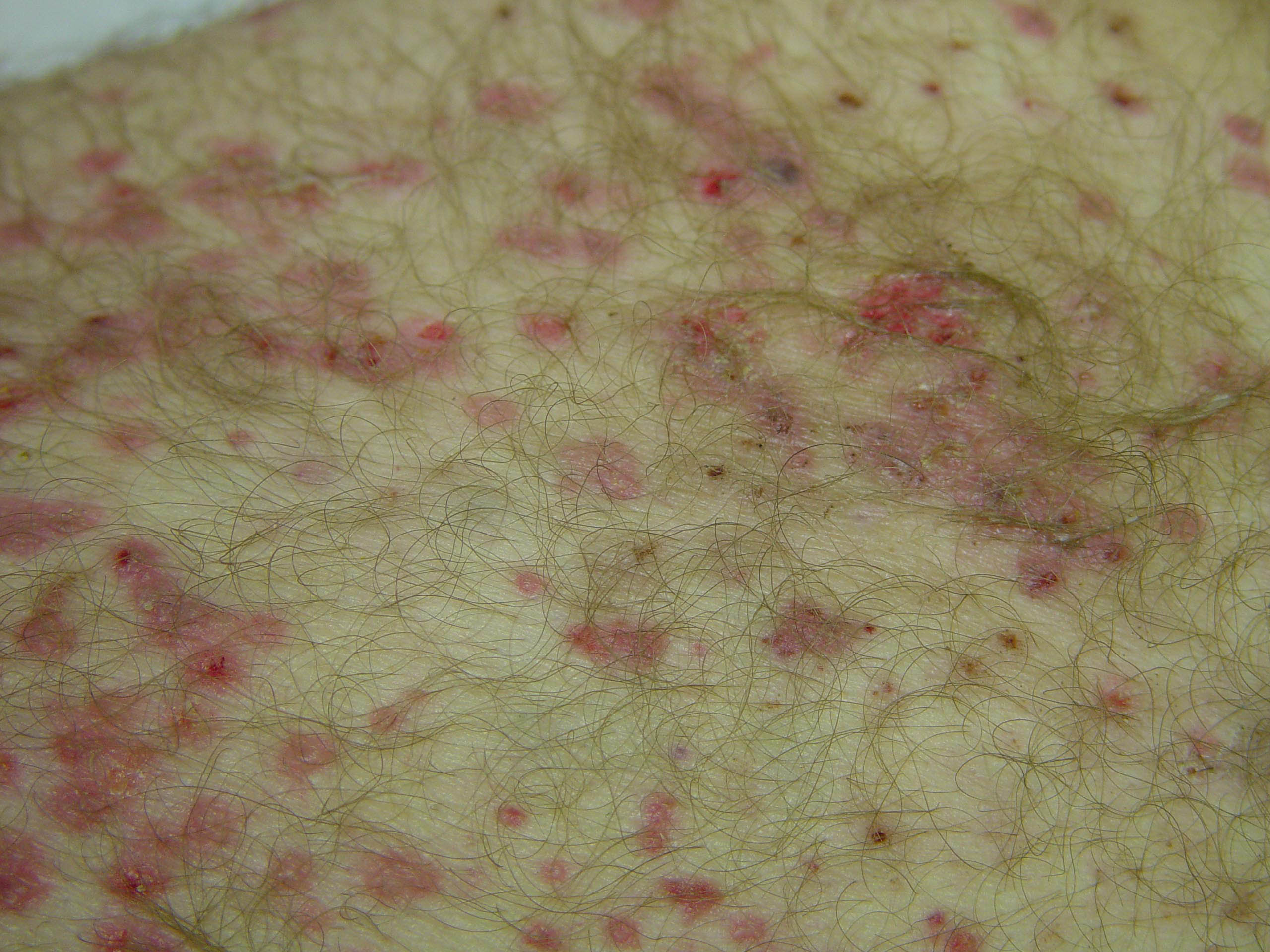
VZV is related closely to herpes simplex viruses (HSVs), with HSV type 1 causing cold sores and HSV type 2 causing genital herpes; all are classified as alpha herpesviruses, a subtype of herpesviruses (Centers for Disease Control and Prevention [CDC], 2007; Harper, Gilbert, & Jeffries, 1998). VZV infection causes two clinically distinct conditions. Primary infection with VZV results in varicella or chickenpox, which largely affects children with a mild, self-limiting course (Wharton, 1996). After clinical resolution of primary infection, viral latent infection is established when VZV retrogrades into the sensory dorsal roots of ganglia (Breuer & Whitley, 2007). Vaccination in children to prevent primary VZV has reduced chickenpox cases in the United States (Marin, Güris, Chaves, Schmid, & Seward, 2007). Herpes zoster, the second clinical condition of VZV infection, results from the reactivation of this latent neurotropic virus and commonly presents with painful, unilateral vesicular skin eruption distributing within the dermatomal zones (Gnann & Whitley, 2002). This column will focus primarily on herpes zoster. Incidence and Risk FactorsAbout one in three Americans will develop zoster during their lifetime, and an estimated one million cases of herpes zoster infections occur in the United States annually (CDC, 2007; Harpaz, Ortega-Sanchez, & Seward, 2008). Age is the most important risk factor, with risk increasing greatly after age 50; about 50% of people who live to age 85 will develop an episode of herpes zoster infection (Harpaz et al.). Women have a slightly higher risk than men, and African Americans have a lower incidence of herpes zoster (Opstelten, Van Essen, Schellevis, Verheij, & Moons, 2006). Altered immunity, particularly cell-mediated immunity, is common among people with cancer; therefore, herpes zoster incidence is significantly higher in older adults with cancer than in the general age-matched population (Rusthoven et al., 1998). Risk varies among different types of cancer and treatments; in patients with solid cancer, herpes zoster incidence is less than 5% but Hodgkin disease incidence is 27.3% (Rusthoven et al.). Among hematopoietic stem cell transplantation recipients, herpes zoster risk is about 13%-55% during the first year; incidence is 5%-17% for solid organ transplantation recipients (Harpaz et al., 2008). Herpes zoster risk also is elevated in patients with HIV or AIDS, chronic inflammatory diseases (e.g., systemic lupus erythematosus), rheumatoid arthritis, Crohn disease and ulcerative colitis, and multiple sclerosis (Harpaz et al.). Mortality for VZV infection in patients who were immunocompromised was 8.7% in one study (Lin & Hadler, 2000). PathogenesisTo date, the pathogenesis of VZV infection is not fully understood because VZW is an exclusively human pathogen and is difficult to replicate in animal models (Breuer & Whitley, 2007). Experiments with severe-combined immunodeficient mice containing human xenografts (e.g., tonsillar tissue, skin, dorsal root ganglia) demonstrated that VZV preferentially infected T cells, particularly CD4 T cells (Ku, Besser, Abendroth, Grose, & Arvin, 2005). During initial viraemia, infected CD4 T cells cause down regulation of the histocompatibility complex class I expression and allow VZV to escape from the immune system (Ku, Padilla, Grose, Butcher, & Arvin, 2002). In addition, infected T cells transport VZV via T-cell trafficking from tonsillar tissue to the skin, where VZV replicates and produces cell-free VZV, resulting in highly infectious skin lesions. Uninfected T cells also arrive at the infection sites, become primed with cell-free VZV, and mount a systemic immune response to control the initial infection (Ku et al., 2005). Following initial infection, the VZV-specific cell-mediated immunity keeps VZV in latency and prevents its reactivation (Breuer & Whitley). When an individual's immune system is compromised, such as in older adults or people with cancer undergoing chemotherapy or transplantation, his or her VZV-specific cell mediated immunity also is likely to be impaired, leading to VZV reactivation. Clinical FeaturesThe two primary clinical manifestations of herpes zoster are rashes and acute neuritis. Patients may experience abnormal skin sensations and a neuropathic type of prodromal pain (e.g., aching, burning, stabbing, itching) prior to the eruption of zoster rashes (see Figure 2). The most common rash sites are the thoracic and lumbar dermatomal zones (Yawn et al., 2007). The rashes initially are erythematous and maculopapular, then progress to coalescing clusters of clear vesicles that contain high concentrations of VZV, which are contagious for VZV seronegative individuals. In immunocompetent people, the rashes crust in 7-10 days and are no longer infectious (Harpaz et al., 2008). Although VZV cutaneous dissemination may start with a dermatomal rash, it presents without any primary dermatomal involvement in some cases. The most common complication following herpes zoster infection is postherpetic neuralgia, a persistent pain that can last months to years and occasionally becomes permanent. Involvement of the ophthalmic branch of trigeminal nerve can lead to herpes zoster ophthalmicus, a serious sight-threatening condition Among immunocompromised populations, herpes zoster rashes typically are more severe and prolonged and may become disseminated, indicating VZV viremia. VZV viremia only occurs among immunocompromised patients (almost 37% of zoster cases) in the absence of antiviral treatment (Gnann & Whitley, 1991; Harpaz et al., 2008). VZV viremia often is accompanied by visceral involvement, which usually is life threatening for immunosuppressed transplantation recipients; the mortality rate is 5%-15%, despite antiviral treatment (Harpaz et al.; Miller & Dummer, 2007). Another life-threatening complication among immunocompromised populations is central nervous system involvement, such as myelitis, VZV encephalitis, ventriculitis, and meningoencephalitis
DiagnosisVZV rashes typically are presented by a well-defined dermatomal distribution in immunocompetent individuals, so the diagnosis can be established by characteristic clinical presentation. However, the clinical presentation may be atypical or may have disseminated disease without rashes in immunocompromised patients; as a result, laboratory tests, including polymerase chain reaction, direct fluorescent antibody, and viral culture are needed to confirm the diagnosis. Polymerase chain reaction assay with specimens from skin lesions, blood, or selected body fluid (e.g., cerebrospinal fluid) can offer the most sensitive results but requires an experienced laboratory (Stranska, Schuurman, De Vos, & van Loon, 2004). However, direct fluorescent antibody offers rapid diagnosis and is highly sensitive (Chan, Brandt, & Horsman, 2001). The specimen is obtained by scraping the bases of uncrusted vesicular skin lesions and placing the scrapings on a plain glass slide. Direct fluorescent antibody is widely available, and its turnaround time for results is fast (about 1.5 hours) compared to VZV viral cultures, which are associated with low yield and require 1-2 weeks of incubation
ManagementAcyclovir, famciclovir, and valacyclovir are nucleoside analogs that inhibit replication of human herpesviruses and are approved by the U.S. Food and Drug Administration for the treatment of herpes zoster. In clinical trials, the agents reduced the viral shedding and duration of skin lesions by promoting rash healing, lessening the severity and duration of acute pain from neuritis, and decreasing the risk for progression to peripheral herpetic neuropathy (Beutner, Friedman, Forszpaniak, Andersen, & Wood, 1995; Dworkin et al., 2007; Tyring et al., 1995, 2000; Wood, Kay, Dworkin, Soong, & Whitley, 1996). Therapy should be initiated within 72 hours of rash onset or as soon as possible (Dworkin et al.) (see Table 1). In patients with herpes zoster ophthalmicus or immunocompromised patients with disseminated VZV infection, IV acylovir 10 mg/kg every eight hours for seven days is recommended. Acylovir can be switched to oral therapy once infection is under control (Dworkin et al.). When acyclovir resistance occurs or is suspected, IV foscarnet 40 mg/kg IV every eight hours for 7-10 days is recommended (Balfour et al., 1994). Doses for IV antiviral agents should be adjusted in patients with renal impairment. Concurrent IV hydration also is recommended because of renal toxicity. Adjunct therapy for pain and postherpetic neuralgia often is required for patients with herpes zoster. Zoster vaccine, a live vaccine, is recommended by the Centers for Disease Control and Prevention in all people aged 60 years and older, except in those with primary or acquired immunodeficiencies (e.g., leukemia, lymphoma, other malignancies affecting the bone marrow or lymphatic system) and AIDS as well as patients on immunosuppressive therapies (Harpaz et al., 2008). Patients whose leukemia is in remission and who have not received chemotherapy or radiation for at least three months can receive zoster vaccine
Reactivation of latent VZV is thought to be linked to a diminished cell-mediated cell immunity (Breuer & Whitley, 2007), particularly diminished CD4-specific cell-mediated cell immunity (Gebo, Kalyani, Moore, & Polydefkis, 2005; Veenstra et al., 1995). The link between CD4 cell counts and VZV reactivation was studied originally among patients with HIV or AIDS in the 1990s (Buchbinder et al., 1992; Gershon et al., 1997; Veenstra et al.). In a study of patients with HIV, the incidence of herpes zoster rose with decreasing CD4 counts: 31.2 events per 1,000 person-years for a CD4 count higher than 500 cells/mcl, 47.2 events per 1,000 person-years for 200-499 cells/mcl, and 97.5 events per 1,000 person-years for less than 200 cells/mcl (Veenstra et al.). In other words, CD4 counts less than 200 cells/mcl are significantly correlated with a higher incidence of VZV reactivation. The median CD4 count at a zoster event is 218 cells/mcl (Gebo et al.). Among patients with cancer, reactivation of VZV has been reported primarily in allogenic bone marrow transplantation (BMT) recipients (Doki et al., 2004; Koc et al., 2000; Steer et al., 2000; Wacker, Hartmann, Benhamou, Salloum, & Lemerle, 1989). An estimated 30%-40% of allogeneic BMT recipients will develop VZV infection during the first year following BMT if the recipients do not receive prolonged VZV prophylaxis (Steer et al.), and almost 20%-50% of the VZV infections will be disseminated VZV (Doki et al.). Long-term acylovir 800 mg BID or low-dose acylovir 400 mg daily was found to be effective in preventing reactivation of VZV in transplantation recipients (Boeckh, Kim, Flowers, Meyers, & Bowden, 2006; Thomson et al., 2005). A retrospective analysis of 192 allogeneic peripheral blood stem cell transplantation recipients indicated that a very low dose of acylovir (200 mg daily) protected against VZV reactivation (Kim et al., 2008). Similarly, 137 BMT recipients who were given long-term acylovir of 200 mg daily until the end of immune suppression and at least one year following BMT had significantly decreased incidence of VZV reactivation, and visceral dissemination and serious complications were completely eliminated (Asano-Mori et al., 2008).
Since VZV prophylaxis has been shown to effectively decrease the incidence of VZV reactivation and reduce disseminated VZV infection in BMT recipients, VZV prophylaxis should be considered for hematologic patients without BMT with severe myelosuppression. Monitoring CD4 counts may be useful for clinicians in determining the need for VZV prophylaxis among high-risk populations, such as (a) hematologic patients with cancer following cytotoxic chemotherapy who fail to recover from myelosuppression over a prolonged period of time, (b) patients with myelodysplastic syndrome who have severe leukopenia refractory to granulocyte-colony-stimulating factor or granulocyte- macrophage-colony-stimulating factor, and (c) patients anticipating a prolonged course of immunosuppressive therapy who also are VZV seropositive (indicting a latent VZV state). If patients' CD4 counts are below 200 cells/mcl, administering acylovir 800 mg BID, a low dose of 400 mg daily, or a very low dose of 200 mg daily may be considered, as such regimens have been shown to effectively decrease the reactivation and disseminated of VZV infection among transplantation recipients (Asano-Mori et al., 2008; Boeckh et al., 2006; Kim et al., 2008; Thomson et al., 2005). Among high-risk patients without transplantation, reactivation and disseminated VZV infection also can occur. Two patients with solid cancers in the first author's practice developed disseminated VZV infections -- one patient with breast cancer receiving standard adjuvant chemotherapy and one patient with metastatic colorectal cancer who received chemotherapy over four years. Therefore, considering VZV prophylaxis is clinically reasonable to reduce the risk of deadly disseminated VZV infection among high-risk patients with cancer without BMT. In addition, the prophylaxis regimen may decrease patients' physical suffering and associated hospitalizations. Nonetheless, additional investigations are needed to define the actual incidence, morbidity, and mortality of VZV reactivation and disseminated infection, the role of CD4 counts, and the effectiveness of VZV prophylaxis among high risk patients without BMT in the hematologic patients with cancer population. |