| Dermatofibroma = الليفوم الجلدي |
|
|
Dermatofibroma
Dermatofibroma is a common cutaneous nodule of unknown etiology that occurs more often in women. Dermatofibroma frequently develops on the extremities (mostly the lower legs) and is usually asymptomatic, although pruritus and tenderness are not uncommon. The latter feature is seen in a sufficient number of patients to make dermatofibroma the most prevalent of all painful skin tumors. A number of well-described, histologic subtypes of dermatofibroma have been reported. Removal of the tumor is not necessary unless diagnostic uncertainty exists or particularly troubling symptoms are present. PathophysiologyThe precise mechanism for the development of dermatofibroma is unknown. Rather than a reactive tissue change, dermatofibroma seems more likely to be a neoplastic process because of the persistent nature of the lesion and the demonstration that it is a clonal proliferative growth.1 Clonality, of course, by itself, is not necessarily synonymous with a neoplastic process; it has been demonstrated in inflammatory conditions, including atopic dermatitis, lichen sclerosis, and psoriasis.
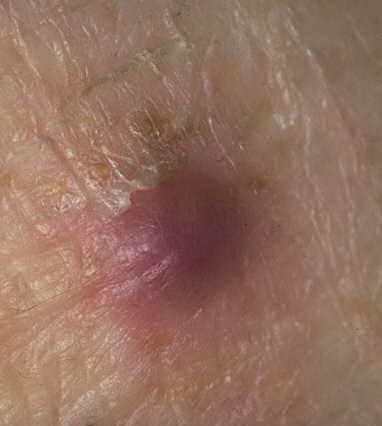
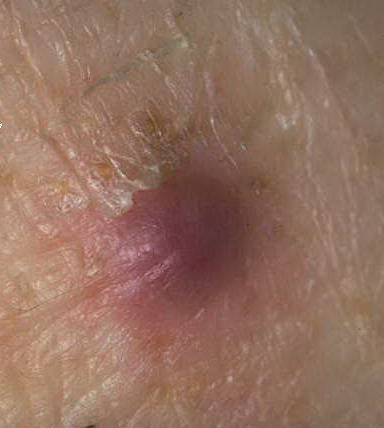
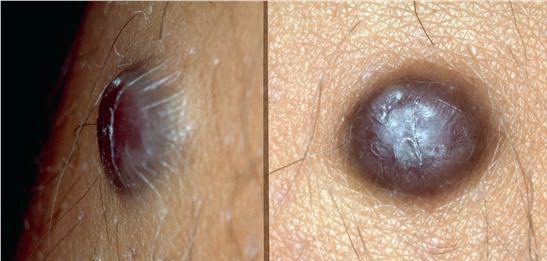
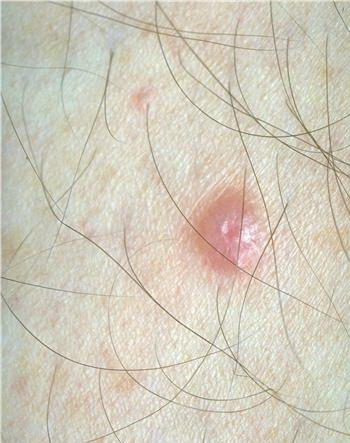
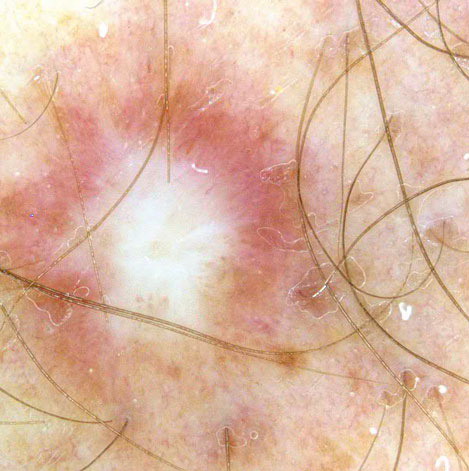
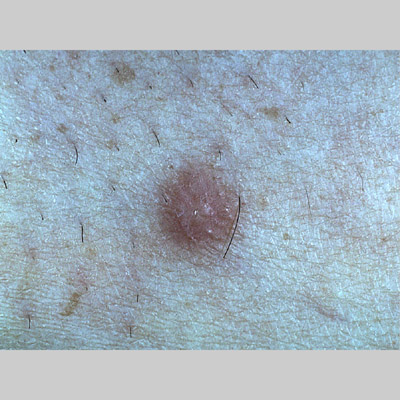
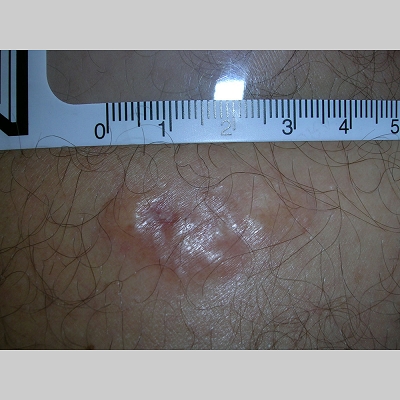
HistoryDermatofibromas typically arise slowly and most often occur as a solitary nodule on an extremity, particularly the lower leg, but any cutaneous site is possible. Several lesions may be present, but only rarely are multiple (ie, 15 or more) tumors found. This multiple variant is seen most frequently in the setting of autoimmune disease or altered immunity, such as systemic lupus erythematosus, Graves disease,10 , Down syndrome,11 , HIV infection, or leukemia and may be indicative of worsening immunoreactivity. PhysicalTypically, the clinical appearance of dermatofibroma is a solitary, 0.5- to 1-cm nodule. A sizable minority of patients may have several lesions, but rarely are more than 15 lesions present. The overlying skin can range from flesh to gray, yellow, orange, pink, red, purple, blue, brown, or black, or a combination of hues (see the image below). On palpation, the hard nodule may feel like a frozen pea or a small pebble fixed to the skin surface and is freely movable over the subcutis. Tenderness may be elicited with manipulation of the lesion.
The characteristic tethering of the overlying epidermis to the underlying lesion with lateral compression, called the dimple sign, may be a useful clinical sign for diagnosis.17 The dimple sign is not unique to dermatofibroma, and dermatoscopy may be useful in supporting the clinical impression.18 CausesHistorically attributed to some traumatic insult to the skin (eg, arthropod bite), the cause of dermatofibroma is unknown. Because of its persistent nature, dermatofibroma is probably better categorized as a neoplastic process rather than a reactive tissue change. A study of eruptive dermatofibromas in a kindred suggests that a genetic component may exist.19
Histologic FindingsThe overlying epidermis is usually acanthotic. Pseudoepitheliomatous hyperplasia and a basaloid proliferation may be noted. The hyperplasia may be caused by the action of fibroblasts on epidermal keratinocytes.23 Basal cell carcinomas occurring upon a dermatofibroma have been reported. Increased pigment may be seen, which may be iron or melanin. Most lesions display a grenz zone of normal papillary dermis overlying the tumor. The subcutis typically is preserved, but if involved (especially when a storiform [cartwheel] pattern is observed), be alert to the possibility of the lesion being a dermatofibrosarcoma protuberans (DFSP).
One clinicopathologic classification scheme31 describes the following 4 categories of dermatofibroma: (1) those with architectural peculiarities, such as deep penetrating, atrophic, giant, aneurysmal (angiomatoid), hemangiopericytomalike, palisading, or ossifying variants; (2) cellular/stromal dermatofibromas, such as clear cell, granular cell, myofibroblastic, sclerotic, monster cell, atypical (pseudosarcomatous), elusive (hemosiderotic), cholesterotic (lipidized), and myxoid variants; (3) dermatofibromas with architectural and cellular/stromal changes in homogeneous arrangement, including epithelioid cell, cellular benign, smooth muscle proliferative, basal cell carcinoma–like, pseudolymphomatous, multinucleate cell angiohistiocytoma, cellular neurothekeoma, plexiform fibrohistiocytic tumor, plexiform xanthoma, and plexiform xanthomatous tumor subtypes; and (4) a complex, composite or combined dermatofibroma category with 2 or more architectural and cellular/stromal patterns in a single lesion. Of the variants listed above, keep in mind that the uncommon sclerotic fibromalike dermatofibroma should be differentiated from sclerotic fibroma. A 2005 study32 showed 7 of 7 of the former lesions to be negative for CD34 and CD99, while 3 of 3 solitary fibromas were positive for CD34 and CD99. For comparison, 14 of 14 "common-type" dermatofibromas in this study were negative for CD34, while 4 demonstrated positivity with CD99. In one study, CD10 was positive in 11 of 11 dermatofibromas and only positive in 1 of 7 epithelioid dermatofibromas, so it was postulated that epithelioid dermatofibroma may be a distinct entity.33 Lichenoid dermatofibroma, ulcerated dermatofibroma, erosive dermatofibroma, diffuse eosinophilic infiltrate dermatofibroma, dermatofibroma accompanied by perforating dermatosis, dermatofibroma with overlying sebaceous hyperplasia, dermatofibroma with intracytoplasmic globules,34 , signet-ring cell dermatofibroma,35 and amyloid light chain deposition36 have also been reported. A case of an apocrine gland cyst with a hemosiderotic dermatofibroma was termed an apocrine hemosiderotic dermatofibroma.37 Induction of adnexal structures by dermatofibroma is quite common and may mimic overlying basal cell carcinoma.38 A 2005 series39 reported the uncommon occurrence of dermatofibroma and melanocytic lesions in the same biopsy specimen. Four of 14 specimens showed the 2 processes to seemingly merge imperceptibly. The lesions included junctional, dermal, and compound nevi as well as a single case of melanoma in situ. Knowledge of this relationship can help prevent rendering the wrong diagnosis and is facilitated by the use of immunohistochemistry, with the melanocytic lesions showing S-100 and Mart-1 positivity with FXIIIa negativity and the dermatofibroma showing S-100 and Mart-1 negativity and FXIIIa positivity. A subsequent case report40 documenting an invasive melanoma occurring in association with a dermatofibroma underscores the role of these immunohistochemical stains. INI-1, present in 100% of dermatofibroma and 13% of epithelioid sarcoma, can help distinguish between these 2 lesions.41
Medical CareNo treatment is usually necessary for dermatofibromas. Simple reassurance that the lesion is benign may be indicated. Intralesional steroid injections have been attempted with variable results. Surgical CareFor cosmetically unacceptable lesions or lesions that are particularly symptomatic, or if any diagnostic uncertainty exists, complete excision, including the subcutaneous fat, is the ideal procedure. An inverted pyramidal biopsy technique may allow for an aesthetically pleasing result, while still providing adequate tissue for histologic findings.42 Superficially shaving the lesion or cryosurgery can be attempted for cosmesis or to decrease the symptoms; however, recurrences are more likely. Carbon dioxide laser treatment of multiple facial dermatofibroma has been reported.43 |