Congential nevus
Congenital nevi are present at birth and result from a proliferation of benign melanocytes in the dermis, epidermis, or both. Occasionally, nevi that are not present at birth but are histologically identical to congenital nevi may develop during the first 2 years of life. This is referred to as congenital nevus tardive.1
Congenital nevi are one of several known risk factors for the eventual development of melanoma. Fortunately, melanoma remains an uncommon malignancy in prepubertal children, with an annual incidence of 0.7 cases per million children aged 0-9 years. Patient concerns regarding changing or worrisome-looking nevi are, nonetheless, very common. Moreover, by the time a child reaches adolescence, the incidence of melanoma increases substantially, with a rate of 13.2 cases per million children aged 15-19 years.2
While many sources have noted the so-called melanoma epidemic in adults, only in recent years have data documented an alarming increase in melanoma in adolescents. This increase, combined with the recognition of clearly identifiable melanoma risk factors in childhood, allows physicians of the 21st century to play a crucial role in the identification of children at risk for melanoma and to aid in the prevention of melanoma through education regarding the risks of ultraviolet light exposure.
The etiology of congenital melanocytic nevi remains unclear. The melanocytes of the skin originate in the neuroectoderm, although the specific cell type from which they derive remains unknown.3,4,5 One hypothesis is that pluripotential nerve sheath precursor cells migrate from the neural crest to the skin along paraspinal ganglia and peripheral nerve sheaths and differentiate into melanocytes upon reaching the skin.6 One possible explanation for the presence of congenital melanocytic nevi is that an external insult results in a mutation that affects the morphogenesis of the embryonic neuroectoderm and migration of precursor cells to the skin.
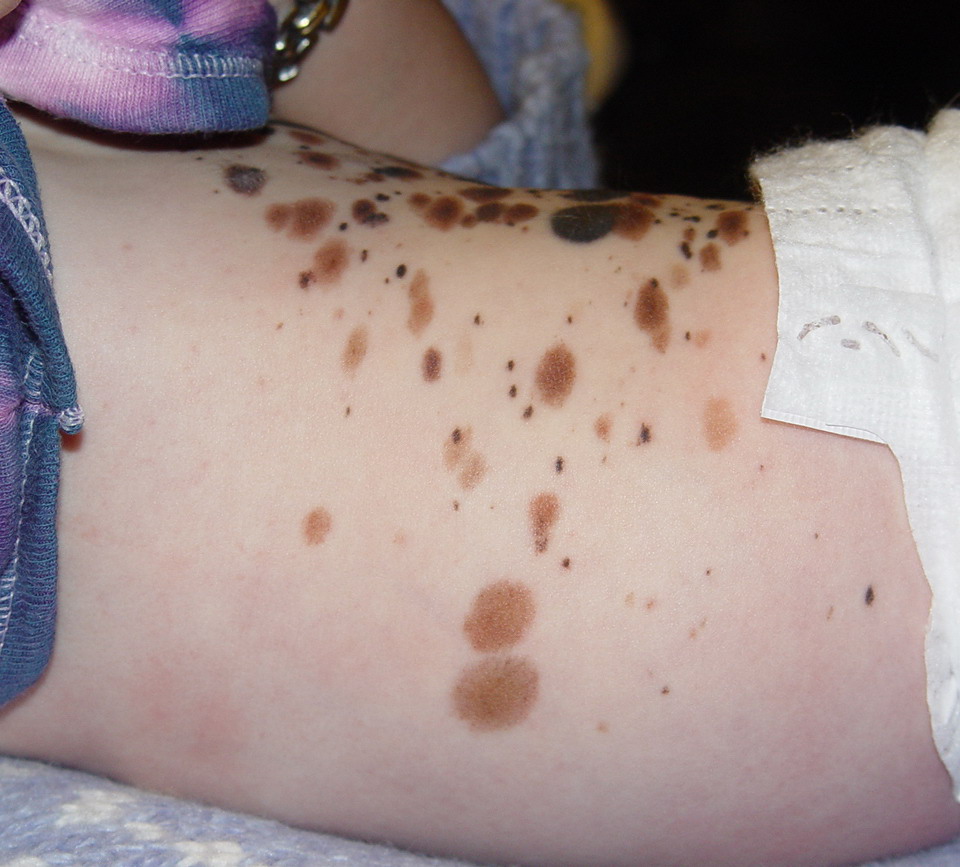
Congenital nevi have been stratified into 3 groups according to size. Small nevi are less than 1.5 cm in greatest diameter, medium nevi are 1.5-19.9 cm in greatest diameter, and large or giant nevi are greater than 20 cm in greatest diameter. Giant nevi are often surrounded by several smaller satellite nevi. An alternate definition is that a small congenital nevus is one for which primary closure is possible after excision.
Congenital nevi may also be seen as a component of neurocutaneous melanosis, a rare congenital syndrome characterized by the presence of congenital melanocytic nevi and melanotic neoplasms of the central nervous system. Rokitansky first described neurocutaneous melanosis in 1861.7 The current diagnostic criteria for neurocutaneous melanosis are (1) large (>20 cm) or multiple (>3) congenital nevi in association with meningeal melanosis or melanoma, (2) no evidence of meningeal melanoma except in patients in whom cutaneous lesions are histologically benign, and (3) no evidence of cutaneous melanoma except in patients in whom meningeal lesions are histologically benign.8
Neurocutaneous melanosis may result from an error in the morphogenesis of the neuroectoderm, which gives rise to the melanotic cells of both the skin and meninges. Clinically, patients may present with increased intracranial pressure due to hydrocephalus or a mass lesion. The prognosis of patients with symptomatic neurocutaneous melanosis is very poor, even in the absence of malignancy. In one review of 39 reported cases of symptomatic neurocutaneous melanosis, death occurred in more than half the patients within 3 years of the onset of neurological symptoms, and most deaths were in patients younger than 10 years.8
Mutations in NRAS in congenital melanocytic nevi can cause mitogen-activated protein kinase activation and may represent early events in melanoma development
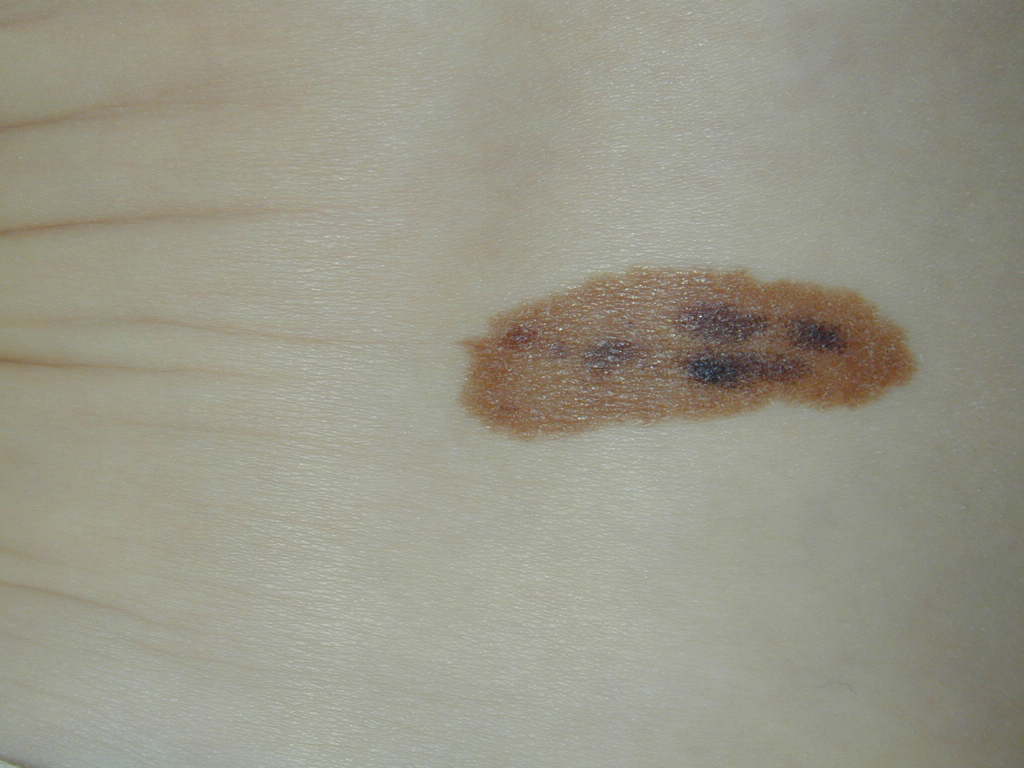
The presence of congenital nevi may be reported by adults, adolescents, or the parents of infants and children.
Nevi may be located anywhere on the body. Classification as a congenital nevus depends in large part on an accurate history or photographs or medical reports from birth.
The etiology of congenital melanocytic nevi has not been elucidated. One possible cause is a mutation due to an external insult.14 An association between infantile hemangiomas and congenital melanocytic nevi has been suggested.15 Future investigation may yield more definitive causative factors
Biopsy confirms a benign or malignant nature in suggestive lesions.
In cases associated with a high index of suspicion for the presence of neurocutaneous melanosis, magnetic resonance imaging of the central nervous system is a useful diagnostic tool. The presence of a large congenital melanocytic nevus in an infant should prompt magnetic resonance imaging testing before age 4 months if it is in a posterior midline location or is associated with multiple satellite nevi.13
A review of dermoscopy patterns in congenital nevi found that most nevi demonstrate a reticular, globular, or reticuloglobular pattern. The findings varied with age and the anatomic location of the nevus, with the globular pattern found more often in younger children and the reticular pattern found in patients aged 12 years or older.17 The clinical trial, The Role of Dermoscopy in the Classification of Melanocytic Nevi, is currently recruiting.
Because of the increased risk of melanoma associated with congenital nevi, attempts have been made to distinguish congenital nevi from acquired nevi on the basis of histology. Distinguishing histologic features include (1) involvement by nevus cells of deep dermal appendages and neurovascular structures (including hair follicles, sebaceous glands, arrector pili muscles, and within walls of blood vessels), (2) extension of nevus cells to deep dermis and subcutaneous fat, (3) infiltration of nevus cells between collagen bundles, and (4) a nevus cell–poor subepidermal zone.18,19,20 Note the images below.
In contrast to congenital nevi, acquired nevi are usually composed of nevus cells that are limited to the papillary and upper reticular dermis and do not involve the appendages.
Medical Care
The management of congenital melanocytic nevi depends on a number of factors, including the size of the lesion, the location of the lesion, the age of patient, the effect on cosmesis, and the potential for malignant transformation.
Although the risk of malignant transformation in small and medium-sized congenital melanocytic nevi has not been established, many physicians agree that the risk is probably not significant enough to warrant the prophylactic removal of all of these lesions. However, some patients may desire removal of these lesions to improve cosmesis.21 Until evidence is presented on which to base definitive treatment guidelines, many physicians are managing small and medium-sized congenital melanocytic nevi with baseline photography and regular follow-up.
Surgical Care
Surgical removal of congenital melanocytic nevi is performed for 2 main reasons, (1) to improve the cosmetic appearance of the patient and (2) to reduce the likelihood of malignant transformation. The increased risk of malignant transformation associated with giant congenital melanocytic nevi is well established. Ideally, these lesions are removed whenever possible. Children with congenital melanocytic nevi of the eyelids and periorbital region may also benefit from early treatment to prevent or minimize disturbance of eyelid function.22 Barriers to removal may include the size of the lesion and its proximity to vital structures. Several different procedures are available to remove congenital melanocytic nevi.23
Surgical excision of giant congenital melanocytic nevi, depending on the size and location of the lesion, may be challenging. Often, the size of the lesion necessitates a staged excision. Tissue expanders, tissue grafts, and tissue flaps are often necessary to close the large defects following excision. Cultured skin replacements have also been used in the closure of surgical wounds.24 Because the melanocytes in such cases may extend deep into underlying tissues (including muscle, bone, and central nervous system), removing the cutaneous component may not eliminate the risk of malignancy.
Curettage of the lesions may be performed during the neonatal period,25 but long-term studies suggest the nevus will, in part, recur. This is likely due to those components of the epidermis that are deep to the level of curettage.
Laser treatment of the lesions has been performed with a number of different types of lasers, including the systems noted below. Because of the lack of penetrance to deeper tissue levels, long-term recurrence is also an issue with these techniques. Laser treatment of congenital melanocytic nevi also remains controversial for a variety of reasons. The effects of sublethal laser fluences on the risk of malignant transformation of melanocytes are uncertain. Additionally, while the destruction of more superficial melanocytes may improve cosmesis, if melanoma does develop in a laser treated lesion, it may be more likely to occur deeper in the tissue where it may evade clinical detection until it reaches a more advanced stage.
- High-energy pulsed carbon dioxide laser
- Erbium:YAG laser
- Normal-mode ruby laser
- Q-switched ruby laser
- Switched alexandrite laser
Because of the risk of neurocutaneous melanosis in patients with giant congenital nevi or multiple smaller congenital nevi, consultation with a neurologist, pediatrician, or both may be useful to detect possible early neurologic manifestations of the disease. Even in the absence of malignancy, neurocutaneous melanosis may cause problems such as obstructive hydrocephalus.
.