| Condyloma acuminatum=اللقموم المؤنف |
|
|
Condyloma acuminatum The viral nature of genital warts was first recognized in 1907 when Ciuffo induced warts after autoinoculation of cell-free wart extracts.1 The human papillomavirus (HPV) was identified with the development of molecular biology techniques as the virus responsible for condyloma acuminatum. Zur Hansen proposed that HPV was likely important in the etiology of genital tract neoplasias in the mid 1970s.2 The DNA of the first genital wart was characterized in 1980. Today, more than 120 distinct HPV subtypes have been identified. This group of viruses is strongly linked to the development of cervical cancer. HPV contributes to 90% of anal cancers and 40% of vulva, vaginal, and penile cancers. Squamous cell carcinoma of the oropharynx is associated with HPV in 50% of cases.3,4
Complete understanding of the natural history of HPV disease has significantly improved over the last 20 years, but key issues remain unanswered. Topics requiring further research include HPV age-specific outcomes, risk of progression and regression of disease, and factors important in the acquisition of immunity following infection.5
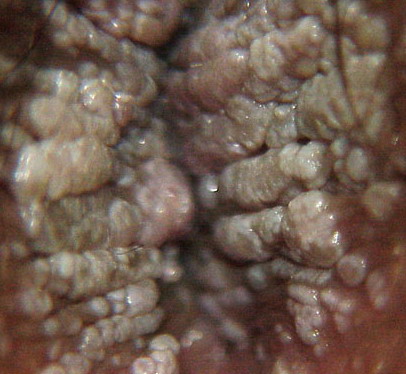
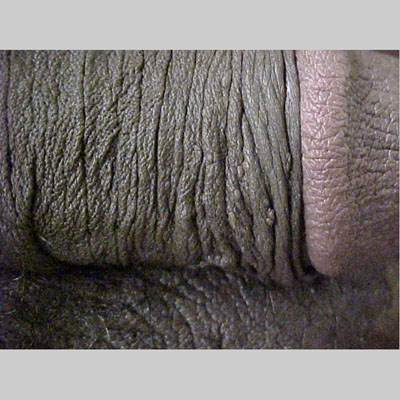
HPV is a group of double-stranded DNA viruses. The genome encodes 6 early open reading frames (E1, E2, E4, E5, E6, E7) and 2 late open reading frames (L1, L2). The E genes encode proteins important in regulatory function, and the L genes encode for viral capsid proteins. This group of viruses can infect many different sites, including the larynx, skin, mouth, esophagus, and the anogenital tract. Approximately 40 different types of HPV can infect the anogenital tract. Infection caused by the HPV virus results in local infections and appears as warty papillary condylomatous lesions. HPV infections in the genital area are sexually transmitted.
HistoryMost patients seek medical care when they notice lumps on the vulva, perianal area, or periclitoral area.
Physical
CausesApproximately 40 different types of HPV can infect the anogenital tract.
HPVs associated with genital tract lesions have been divided into low risk and high risk based on each genotype's association with benign or malignant lesions. Most genital condylomata are due to infection by HPV-6 or HPV-11. These HPV types replicate as an episome and rarely incorporate their genetic material into the host DNA. In contrast, HPV-16 and HPV-18 can be recovered in approximately 70% of squamous cell carcinomas of the cervix. These high-risk HPV types, along with types 31, 33, 45, 51, 52, 56, 58, and 59 incorporate a portion of their genetic material into the host DNA. The E6 and E7 genes can produce oncoproteins that alter cell growth regulation. Specifically, E6 oncoprotein inactivates the tumor suppressor gene p53, and the oncoprotein produced by E7 inactivates pRB (retinoblastoma).
Laboratory StudiesPatients who present with condyloma acuminata do not necessarily need other laboratory studies. Patients who are diagnosed with condyloma are at an increased risk for other STDs.
Imaging StudiesNo imaging studies are indicated. ProceduresPatients who present with typical appearing condyloma acuminata usually do not need a vulvar biopsy. A biopsy is recommended for the following scenarios:
Biopsy technique
Histologic FindingsBiopsy of the vulvar skin associated with condyloma shows evidence of hyperkeratosis, acanthosis, and parakeratosis. A chronic inflammatory infiltrate is often observed within the dermis. Koilocytosis, which is perinuclear cytoplasmic halos, is commonly observed in the superficial epithelial cells. Other microscopic findings include basilar hyperplasia with binucleated and multinucleated cells and enlarged parabasal cells with a foamy nuclear chromatin.
Medical CareA variety of medical treatments are available to remove condyloma acuminata; no single treatment regimen is superior. Patients should be informed that genital warts resolve spontaneously in 20-30% of women within 3 months.12
Medical therapy should be the first option for most patients. The authors' prefer the following 4 options for patient-applied therapy.44
Other options include the following:
Surgical CareSurgical removal of warts is appropriate if the condyloma do not respond to medical therapy, if there are numerous, bulky condyloma, or if the condyloma are associated with vulvar dysplasia. Several options are available.
Activity
No one curative treatment exists for condyloma acuminata.59 Simple topical therapies are the initial treatments of choice for most patients. They are cost effective and result in minimal toxicities. Most result in a 30-90% success rate in eliminating visible condyloma. Many clinical studies using topical therapies are not well designed, making comparisons between therapies difficult. AntimitoticsArrests dividing cells in mitosis, resulting in death of proliferating cells. Podophyllum resin (Podocon-25, Podofin)Treatment results in necrosis of visible wart tissue. Exact mechanism of action is unknown. Great variability exists in the potency of podophyllin between batches. American podophyllum contains one-fourth the amount of the Indian source. Warts visible after 6 treatments usually do not respond to further therapy.60 AdultApply concentration of 25% sparingly onto lesions; wash treatment area 4 h after application; repeat q1-2wk until eliminated PediatricApply as in adults None reported Documented hypersensitivity; diabetes; impaired peripheral circulation; avoid use on mucous membranes, eyes, bleeding warts, moles, birthmarks, or unusual warts with hair PregnancyX - Contraindicated; benefit does not outweigh risk PrecautionsPowerful caustic and severe irritant; do not use if surrounding tissue is swollen or irritated; do not use large amounts; avoid contact with cornea; should be applied by a physician or trained nurse; redness or burning of the skin can occur 6-24 h after treatment Podofilox (Condylox)Topical antimitotic that can be synthesized chemically or purified from plant families Coniferae and Berberidaceae (eg, Juniperus and Podophyllum species). AdultApply 0.5% solution to warts bid for 3 d; repeat qwk for up to 4 wk PediatricApply as in adults None reported Documented hypersensitivity PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsAvoid contact with eyes; if eye contact occurs, immediately flush eye with copious quantities of water and seek medical advice; not for use on mucous membranes of genital area, including urethra, rectum, and vagina; do not exceed frequency of application or duration of usage Antineoplastic agentsTopical preparation containing the fluorinated pyrimidine, 5-fluorouracil. Antineoplastic and antimetabolite agent. Fluorouracil topical (Efudex)Interferes with DNA synthesis by blocking methylation of deoxyuridylic acid, inhibiting thymidylate synthetase and, subsequently, cell proliferation. Limited data exist concerning the efficacy of this therapy for genital warts. Three case series indicate wart clearance in 10-50% of participants.61 Experimental treatments injecting 5-FU with epinephrine and bovine collagen currently are in trials. AdultApply 5% solution to warts 1-3 times per wk; wash off after 8 h PediatricNot established None reported Documented hypersensitivity; potentially serious infections PregnancyX - Contraindicated; benefit does not outweigh risk PrecautionsIncidence of inflammatory reactions may occur with occlusive dressings; porous gauze dressing may be applied for cosmetic reasons without increase in reaction; adjacent healthy skin around warts should be coated with a protective gel before application; reproductive age group should use adequate contraception during therapy DesiccantsThese are acids that are most effective when applied to moist warts. They are nontoxic and can be used in pregnancy. Trichloroacetic acid (Tri-Chlor)Cauterizes skin, keratin, and other tissues. Although caustic, causes less local irritation and systemic toxicity than others in the same class; however, response often is incomplete and recurrence occurs frequently.62 AdultApply 50-85% solution to warts q1-2wk in physician's office; wash off after 4-6 h PediatricAdminister as in adults None reported Documented hypersensitivity; not for use on premalignant or malignant lesions PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsExternal use only; restrict use to treatment areas only; skin adjacent to warts needs to be protected; severe burning may occur Immune response modifiersStimulates production of cytokines and has demonstrated strong antiviral activity. Imiquimod (Aldara)Induces secretion of interferon alpha and other cytokines. Mechanism of action unknown.63 AdultApply 5% cream 3 times per wk hs; leave on skin for 6-10 h; treatment period not to exceed 16 wk PediatricAdminister as in adults None reported Documented hypersensitivity PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsNot recommended for treatment of rectal, cervical, intravaginal, urethral, and intra-anal human papilloma infection; following surgery or drug treatment, do not use topical imiquimod until genital/perianal tissue is healed; local skin erythema, erosion, or abrasion can occur Interferon alfa 2b (Intron)Interferons have been used in the United States for the treatment of genital warts in various doses and preparations. Topical, intralesional, and systemic therapy have been used. Currently, no convincing evidence suggests that topical or systemic therapy is better than placebo.64,65,4,66 Adult1 million U per lesion administered directly into the wart 3 times per wk for 3 wk; no more than 5 warts should be treated at once PediatricAdminister as in adults Theophylline may increase toxicity; cimetidine may increase antitumor effects; zidovudine and vinblastine may increase toxicity Documented hypersensitivity PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsDepression and suicidal ideation may be adverse effects of treatment; flulike symptoms (eg, fever, dizziness, malaise, myalgia, headache) may occur VaccinesA human papillomavirus (HPV) quadrivalent vaccine is now available for prevention of HPV-associated dysplasias and neoplasias, including cervical cancer, genital warts (condyloma acuminata), and precancerous genital lesions. The immunization series should be completed in boys and girls, and young men and women aged 9-26 years. Papillomavirus vaccine (Gardasil)Quadrivalent HPV recombinant vaccine. Adult<26 years: 0.5 mL IM administered as 3 separate doses; administer second and third doses 2 and 6 mo after first dose, respectively Pediatric<9 years: Not established Immunosuppressive therapies (eg, irradiation, antineoplastic agents, corticosteroids) may decrease immune response to vaccine Documented hypersensitivity PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsShake well before administering; administer in deltoid region of upper arm or in higher anterolateral thigh; individuals with impaired immune responsiveness (eg, HIV infection, neoplastic disease, currently taking immunosuppressive drugs) may not elicit antibody response; because of IM administration, do not administer to individuals with bleeding disorders (eg, thrombocytopenia, coagulation disorders, anticoagulant therapy); common adverse effects include pain, swelling, erythema, and/or pruritus at injection site and fever Miscellaneous topical ointmentAnother topical product that has gained FDA approval for genital warts is kunecatechins. Kunecatechins (Veregen)Botanical topical drug product consisting of extract from green tea leaves. Mode of action unknown but does elicit antioxidant activity in vitro. Indicated for topical treatment of external genital and perianal warts (condylomata acuminatum) in immunocompetent patients. AdultApply topically tid; use approximately a 0.5-cm strand of ointment topically for each external genital or perianal wart Pediatric<18 years: Not established |