| Chloasma= الكلف |
|
|
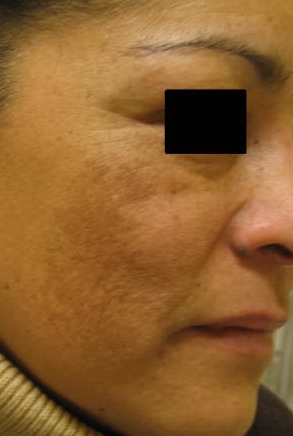
Chloasma
A patchy brown or dark brown skin discoloration that usually occurs on face and may result from hormonal changes, as in pregnancy and during the administration of estrogen containing oral contraceptives. It is generallly found on sun-exposed areas of the face. Melasma often fades over several months after stopping oral contraceptives or hormone replacement therapy(HRT) or after delivering a child. It may return with additional pregnancies or use of these medications. The patches gradually fade over many months. In some people, the discoloration never entirely disappears. However, this condition develops spontaneously in some women who are neither pregnant, taking oral contraceptives, nor HRT medications.
Melasma is a very common skin disorder. Though it can affect anyone, young women with brownish skin tones are at greatest risk. Chloasma is especially common in women aged 20-40. It is more common in dark skins than in fair skins.
Melasma is often associated with the female hormones estrogen and progesterone. It is especially common in pregnant women, women who are taking oral contraceptives ("the pill"), and women taking hormone replacement therapy during menopause.
Sun exposure is also a strong risk factor for melasma. It is particularly common in tropical climates. Melasma develops due to a combination of genetic, hormonal and sun related factors
Melasma has been referred to as the mask of pregnancy because it often develops during pregnancy. Because of melasma’s relation to pregnancy and oral contraceptives, it is thought that estrogen contributes to its development in predisposed persons.
Estrogen is not essential to the development of melasma, however, as men may also be affected A factor that does seem to be essential to the development of melasma is sunlight . Both ultraviolet A (UVA) and ultraviolet B (UVB) are believed to contribute to the formation of melasma in predisposed persons. It may develop in association with menopause, hormonal imbalance and ovarian disorders Melasma may also be triggered by a medication called Dilantin (phenytoin). . It is thought that female sex hormones causes melanocytes or the pigment-producing cells to produce and deposit excess pigments.
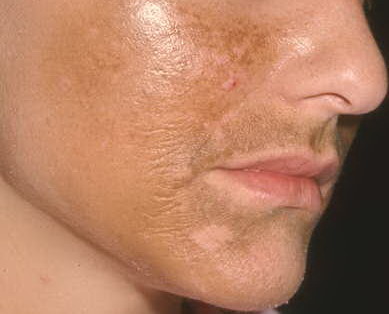
Chloasma usually affects women but occasionally is seen in young men who use after-shave lotions, scented soaps, and other toiletries.
Chloasma is more pronounced during the summer months as a result of sun exposure. It usually fades a few months after delivery. Repeated pregnancies, however, can intensify the pigmentation.
Chloasma also occurs as a side-effect of taking contraceptive pills and injected depot contraceptive preparations. It may also be noticed in apparently healthy, normal, non-pregnant women where it is presumed to be due to some mild and harmless hormonal imbalance.
Sun exposure, following the use of deodorant soaps, scented toiletries, and various cosmetics can also produce this mottled pigmentation. This is called a phototoxic reaction and is due to ultraviolet radiation being absorbed by the chemical substance on the skin.
Deficiency of Folic Acid during pregnancy can also lead to development of Melasma. Melasma during pregnancy is relatively common. Sometimes it is called the "mask of pregnancy." The dark patches typically last until the pregnancy ends. Despite the strong connection to hormones, no one knows exactly what causes the skin discoloration. Other factors that make it more likely that a person will get melasma include using medications that make you sensitive to the sun (photosensitizing). These can include some cosmetics and medicines used to treat ovarian or thyroid problems. If you are already susceptible to melasma, exposure to the sun increases your risk. For example, women who are pregnant or who take a hormone medication and avoid the sun are less likely to develop melasma than are those who spend a lot of time in the sun
Melasma doesn't cause any other symptoms besides skin discoloration but may be of great cosmetic concern. Diagnosis
Conventional Treatment
Creams containing tretinoin, kojic acid, and azelaic acid have been shown to improve the appearance of melasma. Occasionally, doctor may recommend chemical peels or topical steroid creams.
In severe cases, laser treatments can be used to remove the dark pigment. HOMEOPATHY TREATMENT & HOMEOPATHIC REMEDIESHomeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines are selected after a full individualizing examination and case-analysis, which includes the medical history of the patient, physical and mental constitution etc. A miasmatic tendency (predisposition/suceptability) is also often taken into account for the treatment of chronic conditions. The medicines given below indicate the therapeutic affinity but this is not a complete and definite guide to the treatment of this condition. None of these medicines should be taken without professional advice
Homeopathy TherapeuticsSulphur, Lycopodium clavatum, Sepia offincinalis, Thuja occidentalis, Argenticum nitricum, Cadmium sulphuratum, Copaiva offincinalis, Guarana, Caulophyllum, Thalictroides, Plumbum metallicum, Curare.
|