| Cheilitis Granulomatosa of Miescher =التهاب الشفة الحبيبي لميشر |
|
|
Cheilitis Granulomatosa of Miescher
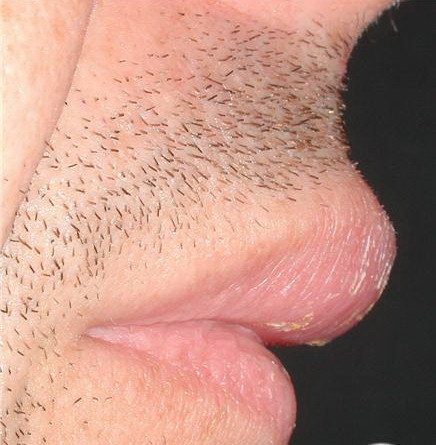
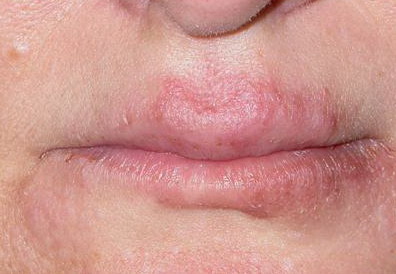
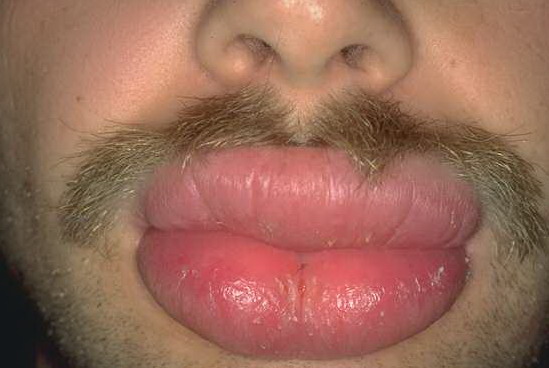
Granulomatous cheilitis is a chronic swelling of the lip due to granulomatous inflammation. Miescher cheilitis is the term used when the granulomatous changes are confined to the lip. Miescher cheilitis is generally regarded as a monosymptomatic form of the Melkersson-Rosenthal syndrome, although the possibility remains that these may be 2 separate diseases. Melkersson-Rosenthal syndrome is the term used when cheilitis occurs with facial palsy and plicated tongue Melkersson-Rosenthal syndrome is occasionally a manifestation of Crohn disease or orofacial granulomatosis (OFG)
Cheilitis granulomatosa is episodic with nontender swelling and enlargement of one or both lips. Occasionally, similar swellings involve other areas, including the periocular region. PhysicalThe earliest manifestation of granulomatous cheilitis is sudden diffuse or occasionally nodular swellings of the lip or the face involving (in decreasing order of frequency) the upper lip, the lower lip, and one or both cheeks. The forehead, the eyelids, or one side of the scalp may be involved (less common). The upper lip is involved slightly more often than the lower lip, and it may feel soft, firm, or nodular on palpation. Once chronicity is established, the enlarged lip appears cracked and fissured with reddish brown discoloration and scaling. The fissured lip becomes painful and eventually acquires the consistency of firm rubber. Swelling may regress very slowly after some years. Regional lymph nodes are enlarged (usually minimally) in 50% of patients. A fissured or plicated tongue is seen in 20-40% of patients. Its presence from birth (in some patients) may indicate a genetic susceptibility. Patients may lose the sense of taste and have decreased salivary gland secretion. Facial palsy of the lower motor-neuron type occurs in about 30% of patients. Facial palsy may precede attacks of edema by months or years, but it more commonly develops later. Facial palsy is intermittent at first, but it may become permanent. It can be unilateral or bilateral, partial or complete. Other cranial nerves (eg, olfactory, auditory, glossopharyngeal, hypoglossal) are occasionally affected. CausesThe cause of granulomatous cheilitis is unknown.10 A genetic predisposition may exist in Melkersson-Rosenthal syndrome; siblings have been affected, and a plicated tongue may be present in otherwise unaffected relatives. Crohn disease, sarcoidosis, and orofacial granulomatosis may present in a similar clinical fashion, and with identical histologic findings. Dietary or other antigens are the most common identified cause of orofacial granulomatosis (OFG).11,12 Contact antigens are sometimes implicated.13 OFG may result from reactions to some foods or medicaments, such as cinnamon aldehyde and benzoates .
Laboratory StudiesSerum angiotensin-converting enzyme test may be performed to help exclude sarcoidosis. Patch tests may be used to help exclude reactions to metals, food additives, or other oral antigens. Some cases may be associated with such sensitivities. If found, avoidance of the implicated allergen is recommended. Imaging StudiesGastrointestinal tract endoscopy, radiography, and biopsy may be used to help exclude Crohn disease. Chest radiography or gallium or positron emission tomography (PET) scanning may be performed to help exclude sarcoidosis and tuberculosis. Panorex dental films may be obtained to assess for the presence of a chronic dental abscess
Histologic FindingsHistologic changes are not always conspicuous or specific in many cases of long duration; the infiltrate becomes denser and pleomorphic, and small focal granulomas are formed that are indistinguishable from Crohn disease or sarcoidosis. Small granulomas occur in the lymphatic walls in some cases. Similar changes may be present in cervical lymph nodes
Medical CareSimple compression for several hours daily may produce significant improvement. Compression devices may reduce lip edema. Orofacial granulomatosis may improve with implementation of a cinnamon- and benzoate-free diet. Intralesional corticosteroids may be helpful in some patients.15 Success with other treatments has been reported anecdotally. None of the agents listed below has been systematically evaluated. Immunomodulatory agents are as follows:
Antimicrobials are as follows:
Surgical CareSurgery and radiation have been used. Surgery alone is relatively unsuccessful. Reduction cheiloplasty with intralesional triamcinolone and systemic tetracycline offer the best results.23 Give corticosteroid injections periodically after surgery to avoid an exaggerated recurrence. ConsultationsConsult a gastroenterologist, an immunologist, and an oral medicine specialist. MedicationClofazimine or metronidazole may produce resolution in granulomatous cheilitis. Intralesional corticosteroid (triamcinolone) injections may reduce swelling. Systemic corticosteroids are rarely indicated and not all cases respond. Azathioprine, dapsone, sulfapyridine, or sulfasalazine may be helpful. Long-term penicillin, tetracycline, erythromycin, and ketotifen are other management approaches that are occasionally helpful. No randomized controlled trials have yet been recorded with possible therapies such as tacrolimus, thalidomide, or infliximab. AntibioticsTherapy must be comprehensive and should cover all likely pathogens in the clinical setting. Clofazimine (Lamprene 50- or 100-mg cap)Inhibits mycobacterial growth, binds preferentially to mycobacterial DNA. Has antimicrobial properties, but mechanism of action is unknown.
Adult100 mg PO bid for 10 d, then twice weekly for 4 mo Pediatric1 mg/kg/d PO qd Dapsone may inhibit anti-inflammatory activity Documented hypersensitivity; breastfeeding; hepatic disease; renal disease PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsSevere abdominal symptoms may require exploratory laparotomies; caution in patients with GI problems (eg, abdominal pain, diarrhea); skin discoloration due to drug may result in depression or suicide; apply oil to skin for dryness and ichthyosis; stains soft contact lenses Dapsone (Avlosulfon)Bactericidal and bacteriostatic against mycobacteria. Mechanism of action is similar to that of sulfonamides where competitive antagonists of PABA prevent formation of folic acid, inhibiting bacterial growth.
Adult50-300 mg PO qd (average dose, 100 mg qd) PediatricNot established May inhibit anti-inflammatory effects of clofazimine; hematologic reactions may increase with folic acid antagonists, eg, pyrimethamine (monitor for agranulocytosis during second and third mo of therapy); probenecid increases toxicity; trimethoprim with dapsone may increase toxicity of both drugs; because of increased renal clearance, levels may significantly decrease when administered concurrently with rifampin Absolute: Documented hypersensitivity PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsPerform weekly blood counts (first mo), then perform WBC counts monthly (6 mo), and then semiannually; discontinue if significant reduction in platelets, leukocytes, or hematopoiesis occurs; caution in methemoglobin reductase deficiency, G-6-PD deficiency, or hemoglobin M because of high risk for hemolysis and Heinz body formation; caution in patients exposed to other agents or conditions (eg, infection, diabetic ketosis) capable of producing hemolysis; peripheral neuropathy can occur (rare); phototoxicity may occur when exposed to UV light Anti-inflammatoriesThese agents decrease inflammatory responses and systemically interfere with events leading to inflammation. Sulfapyridine (Dagenan)Competitive antagonist of PABA. Mechanism of action in linear IgA dermatosis is unknown.
AdultInitial dose is 500 mg PO bid; increase by 1 g q1-2wk until disease is controlled; control may require 1-4 g/d Pediatric35 mg/kg PO bid; not to exceed 100 mg/kg/d Bioavailability of digoxin is reduced (interval of 2-3 h between administrations is recommended) Documented hypersensitivity; slow acetylators may require smaller doses or more gradual initial dosage adjustment PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsIdiosyncratic reactions, such as hypersensitivity pneumonitis, a lupuslike syndrome, pancreatitis, and toxic hepatitis, may occur; agranulocytosis rarely occurs; both immune hemolytic anemia and nonimmune hemolytic anemia develop (the latter is more common in patients with G-6-PD deficiency); folate deficiency may occur secondary to impaired absorption; nephrolithiasis may occur as with other sulfa drugs; toxic epidermal necrolysis has been reported with medications containing sulfa groups; check CBC count and liver function tests monthly for 5 mo then q6wk thereafter Sulfasalazine (Azulfidine)Decreases inflammatory response and systemically inhibits prostaglandin synthesis.
Adult500 mg PO qd PediatricNot established Decreases effects of iron, digoxin, and folic acid; conversely, increases effect of oral anticoagulants, oral hypoglycemic agents, and methotrexate Documented hypersensitivity; sulfa drugs or any component; those diagnosed with GI or GU obstruction PregnancyB - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals PrecautionsCaution in patients with renal or hepatic impairment, blood dyscrasias, or urinary obstruction CorticosteroidsThese agents have anti-inflammatory properties and cause profound and varied metabolic effects. In addition, these agents modify the body's immune response to diverse stimuli. Triamcinolone (Aristocort)For inflammatory dermatosis responsive to steroids. Decreases inflammation by suppressing migration of polymorphonuclear leukocytes and reversing capillary permeability.
Adult2.5-40 mg (10 mg/mL or 40 mg/mL formulations; intralesional); repeat prn but not to exceed q4-6wk Pediatric2.5-15 mg (10 mg/mL or 40 mg/mL solutions; intralesional); repeat prn but not to exceed q4-6wk None reported Documented hypersensitivity; fungal, viral, and bacterial skin infections PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsDo not use in decreased skin circulation; prolonged or frequent use may result in Cushing syndrome, reversible HPA-axis suppression, hyperglycemia, and glycosuria ImmunosuppressantsThese agents inhibit key factors that mediate immune reactions, which, in turn, decrease inflammatory responses. Azathioprine (Imuran)Antagonizes purine metabolism and inhibits synthesis of DNA, RNA, and proteins. May decrease proliferation of immune cells, which results in lower autoimmune activity.
Adult1 mg/kg qd/bid (empiric) or by TPMT level; increase by 0.5 mg/kg q4wk until response, not to exceed 2.5 mg/kg/d PediatricSafety and efficacy not established Allopurinol increases risk of pancytopenia; captopril/ACE inhibitors may increase risk of anemia and leukopenia; warfarin dose may need to be increased; pancuronium dose may need to be increased for adequate paralysis; live virus vaccines and cotrimoxazole increase risk of hematologic toxicity; rifampicin may cause transplants to possibly be rejected; clozapine may increase risk of agranulocytosis Absolute: Documented hypersensitivity, pregnancy or attempting pregnancy, clinically significant active infection PregnancyD - Fetal risk shown in humans; use only if benefits outweigh risk to fetus PrecautionsIncreased risk of neoplasia; caution in liver disease and renal impairment; hematologic toxicities may occur; rarely, patients may develop fever without associated infections; measure thiopurine methyltransferase level prior to treatment; periodically monitor CBC count and liver function |