| Collodian baby=الطفل الكوللوديوني |
|
|
Collodion Baby
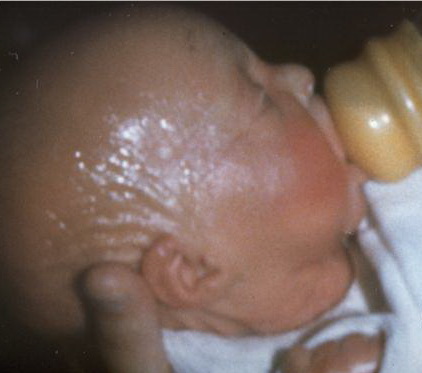
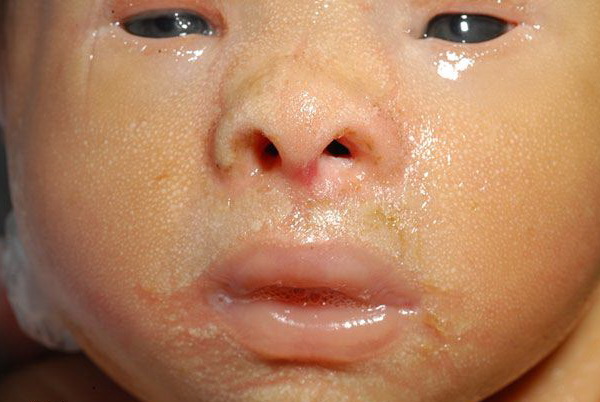
A collodion baby is the usual presentation of ARCI . Less commonly, a collodion presentation can also be seen in infants with several other forms of ichthyosis and, rarely, Gaucher disease . The child is born encased in a translucent, parchment-like membrane that is taut and may impair respiration and sucking. The spectrum of involvement is probably variable, but has not been well characterized. In addition, the birth is often premature, which adds to morbidity. During the first 2 weeks of life, the membrane breaks up and peels off, often leaving fissures, with impairment of the barrier to infection and water loss. This can lead to difficulties in thermal regulation, an increased risk of infection, and hypernatremic dehydration. Newborn care should include careful monitoring of temperature, hydration, electrolytes, and for infection. Measures to keep the peeling membrane soft and lubricated to facilitate flexibility and desquamation should be used. Appropriate pain management and eye care should be employed, when indicated. These newborns usually benefit from a humidified incubator where the air is saturated with water; wet compresses followed by bland lubricants can be used to further hydrate the membrane and achieve maximum pliability.68 If, during peeling, residual areas of the membrane are allowed to dry and harden in areas such as the extremities, the taut membrane can constrict and lead to distal swelling. Collodion presentation can develop into a wide spectrum of ichthyotic phenotypes as the child grows . In addition, an autosomal recessive, self-healing collodion baby has been described, where the skin clears within the first few weeks and transitions into normal skin thereafter. A TGM1 mutation sensitive to increase hydrostatic pressure (such as might be found in utero) has been found in one family with two affected children with a history of self-healing collodion membranes.
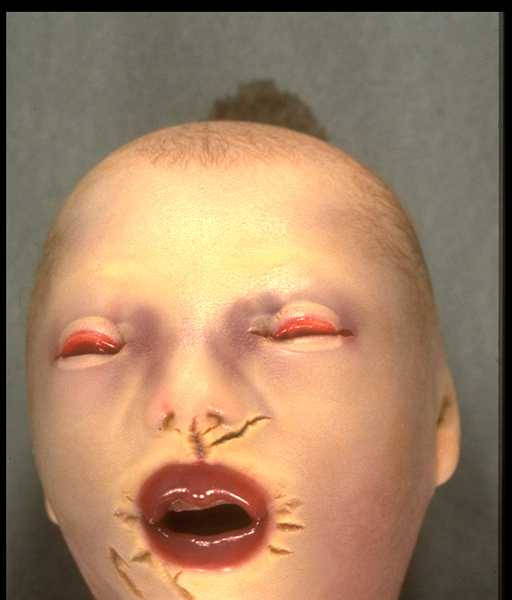
The newborn affected with one of the more severe, generalized types of epidermolytic hyperkeratosis usually has erythema, blistering, widespread erosions, and denuded skin. Because there is a high frequency of new mutations, the disease may be unexpected, and the diagnosis may be unknown. Epidermolysis bullosa or staphylococcal scalded-skin syndrome may be suspected, and the infant treated with antibiotics. The newborn may require intensive care with fluid and electrolyte monitoring. Specialized skin care can minimize blistering and enhance healing of erosions and should include lubrication (to decrease friction as well as mechanical trauma), protective padding, and specialized wound dressings. The newborn with extensive erosions is prone to bacterial infection and sepsis, and carefully chosen topical and systemic antibiotics can minimize the extent of infection. Harlequin Ichthyosis A dramatic, severe, and often fatal presentation of ichthyosis is that of harlequin ichthyosis . The child is often premature and born with massive, shiny plates of stratum corneum separated by deep, red fissures that tend to form geometric patterns, as seen in the patched costumes of the harlequin clowns from the Italian Commedia dell'Arte dating from the sixteenth and seventeenth centuries. There are poorly developed or absent ears and marked ectropion and eclabium. The first report is from the diary of Rev. Oliver Hart, of Charleston, South Carolina, who described these features in 1750. These children are at great risk during the neonatal period and often die shortly after birth. Abnormal water loss through the skin and poor temperature regulation lead to risk of fluid and electrolyte imbalance. The infants are also at risk for infection beginning in the skin, but at the same time (because of poor temperature regulation) do not show the usual signs of infection. Normal respiration may be restricted by the taut skin. Treatment
In harlequin ichthyosis, normal lamellar granules are not found; instead, there are small vesicles that lack internal structure. There is also no evidence of the lipid lamellae that form between granular and cornified cells as a result of discharge of lamellar granule contents into the intercellular space. Occurrence of harlequin ichthyosis in consanguineous families suggests autosomal recessive inheritance. Mutations in ABCA12, which codes for an adenosine triphosphatebinding cassette transporter involved in lamellar granule secretion and epidermal lipid transport, have been shown to underlie harlequin ichthyosis. Mutations in ABCA12 have also been identified in a subset of individuals with ARCI .
|