BULLOUS IMPETIGO
.
Three types of skin eruptions can be produced by phage group II S. aureus, particularly strains 77 and 55: (1) bullous impetigo, (2) exfoliative disease (SSSS), and (3) nonstreptococcal scarlatiniform eruption (staphylococcal scarlet fever). All three represent varying cutaneous responses to extracellular exfoliative toxins (“exfoliatin”) types A and B produced by these staphylococci . Exfoliative toxin A acts as a serine protease of desmoglein 1, the desmosomal cadherin that is also the target of autoantibodies in pemphigus foliaceus.
In a study of bullous impetigo, 51 percent of patients had concurrent S. aureus cultured from the nose or throat, and 79 percent of cultures grew the same strain from both sites.
Cutaneous Lesions
.
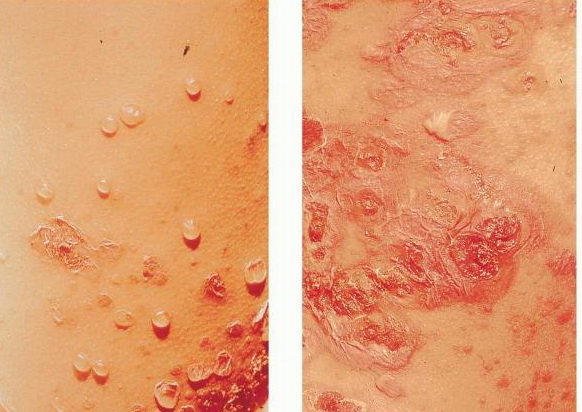
Bullous impetigo occurs more commonly in the newborn and in older infants, and is characterized by the rapid progression of vesicles to flaccid bullae . Decades ago, extensive bullous impetigo (archaic term: pemphigus neonatorum or Ritter disease) occurred in epidemics within neonatal nurseries.
Bullae usually arise on areas of grossly normal skin. The Nikolsky sign (sheet-like removal of epidermis by shearing pressure) is not present. Bullae initially contain clear yellow fluid that subsequently becomes dark yellow and turbid , and their margins are sharply demarcated without an erythematous halo. The bullae are superficial, and within a day or two, they rupture and collapse, at times forming thin, light-brown to golden-yellow crusts . So-called bullous varicella represents superinfection by S. aureus (phage group II) of varicella lesions (bullous impetiginization).
Laboratory Tests.
Gram stain of exudates from bullous impetigo reveals Gram-positive cocci in clusters. S. aureus belonging to phage group II can be cultured from the contents of intact bullae.
Histologically, the lesions of bullous impetigo show vesicle formation in the sub-corneal or granular region, occasional acantholytic cells within the blister, spongiosis, edema of the papillary dermis, and a mixed infiltrate of lymphocytes and neutrophils around blood vessels of the superficial plexus.
Differential Diagnosis.
See Box 177-2 for differential diagnosis of bullous impetigo.
Box 177-1 Differential Diagnosis of Non-Bullous Impetigo
Consider
· Seborrheic dermatitis
· Atopic dermatitis
· Allergic contact dermatitis
· Epidermal dermatophyte infections
· Tinea capitis
· Herpes simplex
· Varicella
· Herpes zoster
· Scabies
· Pediculosis capitis
Always Rule Out
· Herpes simplex
· Herpes zoster
· Scabies
PROGNOSIS AND CLINICAL COURSE.
Untreated, invasive infection can complicate S. aureus impetigo with cellulitis, lymphangitis, and bacteremia, resulting in osteomyelitis, septic arthritis, pneumonitis, and septicemia. Exfoliatin production can lead to SSSS in infants and in adults who are immunocompromised or have impaired renal function.
TREATMENT.
Local treatment with mupirocin ointment or cream, removal of crusts, and good hygiene is sufficient to cure most mild to moderate cases Systemic antibiotics may be required in extensive cases. The frequency of isolation of group A streptococcus makes such therapy a reasonable approach in most patients who have a significant degree of involvement. There is no role for general disinfectant treatments or bacitracin.
Staphylococcal impetigo responds quite promptly to appropriate treatment. In an adult with extensive or bullous lesions, dicloxacillin (or similar penicillinase-resistant semi-synthetic penicillin), 250 to 500 mg orally (PO) four times daily (qid), or erythromycin (in the penicillin-allergic patient), 250 to 500 mg PO qid, should be given. Treatment should be continued for 5 to 7 days (10 days if streptococci are isolated). Also, a single course of oral azithromycin (in adults 500 mg on the first day, 250 mg daily on the next 4 days) has been shown to be equally as effective as dicloxacillin for skin infections in adults and children. For impetigo caused by erythromycin-resistant S. aureus, which is commonly isolated from impetigo lesions of children, amoxicillin plus clavulanic acid [25 mg/kg/day given three times a day (tid)],
cephalexin (40 to 50 mg/kg/day), cefaclor (20 mg/kg/day given tid), cefprozil (20 mg/kg once daily), or clindamycin (15 mg/kg/day tid or qid) given for 10 days are effective alternative therapies.