Leprosy is a chronic granulomatous disease principally affecting the skin and peripheral nervous system. Leprosy is caused by infection with Mycobacterium leprae. Although much improved in the last 25 years, knowledge of the pathogenesis, course, treatment, and prevention of leprosy continues to evolve. The skin lesions and deformities were historically responsible for the stigma attached to leprosy. However, even with proper multidrug therapy (MDT), the consequent sensory and motor damage results in the deformities and disabilities associated with leprosy.
The earliest description of leprosy comes from India around 600 BCE. Leprosy was then described in the Far East around 400 BCE. In the fourth century, leprosy was imported into Europe, where its incidence peaked in the 13th century. Leprosy has now nearly disappeared from Europe. Affected immigrants spread leprosy to North America.
Armauer Hansen discovered M leprae in Norway in 1873. M leprae was the first bacillus to be associated with human disease. Despite this discovery, leprosy was not initially thought to be an infectious disease.
In 2009, the discovery of a new cause of leprosy, Mycobacterium lepromatosis, was announced. Genetically, M leprae and M lepromatosis are very similar, but M lepromatosis causes the diffuse form lepromatous leprosy found in Mexico and the Caribbean.1
Humans are the primary reservoir of M leprae. Animal reservoirs of leprosy have been found in 3 species: 9-banded armadillos, chimpanzees, and mangabey monkeys.
Other eMedicine articles on leprosy include Leprosy (Neurology), Neuropathy of Leprosy, and Leprosy (Infectious Diseases).
Pathophysiology
Leprosy is not a highly infectious disease. The principal means of transmission is by aerosol spread from infected nasal secretions to exposed nasal and oral mucosa. Leprosy is not generally spread by means of direct contact through intact skin, although close contacts are most vulnerable. The incubation period for leprosy is 6 months to 40 years or longer. The mean incubation period is 4 years for tuberculoid leprosy and is 10 years for lepromatous leprosy.
The areas most commonly affected by leprosy are the superficial peripheral nerves, skin, mucous membranes of the upper respiratory tract, anterior chamber of the eyes, and the testes. These areas tend to be cool parts of the body. Tissue damage depends on the degree to which cell-mediated immunity is expressed, the type and extent of bacillary spread and multiplication, the appearance of tissue-damaging immunologic complications (ie, lepra reactions), and the development of nerve damage and its sequelae.
M leprae is an obligate intracellular, acid-fast, gram-positive bacillus with an affinity for macrophages and Schwann cells. For Schwann cells in particular, the mycobacteria bind to the G domain of the alpha-chain of laminin 2 (found only in peripheral nerves) in the basal lamina. Their slow replication within the Schwann cells eventually stimulates a cell-mediated immune response, which creates a chronic inflammatory reaction. As a result, swelling occurs in the perineurium, leading to ischemia, fibrosis, and axonal death
Laboratory Studies
- Skin biopsy
- The presence of an inflamed nerve in a skin biopsy specimen is considered the criterion standard for diagnosis.
- The skin biopsy sample should be examined for morphologic features and for the presence of acid-fast bacilli. Biopsy is useful for determining the morphologic index, which is used in the evaluation and treatment of patients. The morphologic index is the number of viable bacilli per 100 bacilli in the leprous tissue. The bacterial index of granuloma (BIG) does not differentiate between viable and nonviable bacilli.25
- See Histologic Findings below.
- Lepromin testing
- This test indicates host resistance to Mycobacterium leprae. Its results do not confirm the diagnosis, but they are useful in determining the type of leprosy.
- A positive finding indicates cell-mediated immunity, which is observed in tuberculoid leprosy. A negative finding suggests a lack of resistance to disease and is observed in patients with lepromatous leprosy. A negative result also indicates a worsened prognosis.
- To perform this test, bacillary suspension is injected into the forearm. An assessment of the reaction at 48 hours is called the Fernandez reaction, and a positive result indicates delayed hypersensitivity to antigens of M leprae or mycobacteria that cross-react with M leprae. When the reaction is read at 3-4 weeks, it is called the Mitsuda reaction, and a positive result indicates that the immune system is capable of mounting an efficient cell-mediated response.
- Serology and polymerase chain reaction (PCR) testing: Although useful in detecting multibacillary disease, these are not widely performed because they fail to reliably detect early or mild forms of leprosy.
- Serology can be used to detect antibodies to M leprae –specific phenolic glycolipid-I (PGL-I). This test is useful primarily in patients with untreated lepromatous leprosy, because 90% of patients have antibodies. However, antibodies are present in only 40-50% of patients with paucibacillary disease. PGL-I antibody levels decline significantly during MDT; therefore, these levels may be monitored for chemotherapy effectiveness.26
- A dipstick assay test called the M leprae lateral flow test can detect PGL-I antibodies within 10 minutes with a sensitivity of 90-97.4% in multibacillary leprosy patients. It has the added advantages of using whole blood (versus serum), the technique is easily taught, the results are easily interpreted, and it requires no special equipment.27
- The use of the anti–45-kd and modified anti-PGL-I antibody assays in combination may be more sensitive in detecting cases of paucibacillary leprosy than either assay individually.28
- PCR analysis targeting 16s ribosomal RNA can be used to detect and identify M leprae. The technique is used most often when acid-fast bacilli are detected but clinical or histopathologic features are atypical. Specimens for PCR should be fixed in alcohol or should be rapidly processed because prolonged formalin fixation decreases the sensitivity.29
- The development of a one-step reverse transcriptase PCR assay may be more sensitive in detecting bacilli in slit smears and skin biopsy specimens. This RNA-based assay is also effective for monitoring bacteria clearance during therapy.30
- Other: Although laboratory studies help in making a definitive diagnosis of leprosy, such tests are usually unavailable in remote areas and in some developing countries.
Imaging Studies
- Radiographs
- Plain radiographs may be useful to detect and monitor leprosy-induced bone changes.31
- Resorption, fragmentation, and maligned fractures are common signs of leprosy-induced bone changes. Medullary sclerosis or wavy diaphyseal borders indicate diaphyseal whittling.
Histologic Findings
In the indeterminate form, findings are nonspecific. Histiocytes and lymphocytes are scattered, with some concentration around dermal appendages and nerves. At times, an acid-fast bacillus can be observed in a nerve bundle. The number of dermal mast cells may be increased.
In the tuberculoid form of leprosy, well-developed epithelioid granulomas are observed in the papillary dermis, often around neurovascular structures. The granulomas are surrounded by lymphocytes, which extend into the epidermis. Langhans giant cells are common. Dermal nerves are destroyed or swollen because of the granulomas. Acid-fast bacilli are not observed. S-100 is useful in identifying nerve fragmentation and differentiating it from other granulomatous disease.32
In the borderline tuberculoid form, well-developed epithelioid cell granulomas are apparent and diffuse, but few or no Langhans giant cells are observed. Few lymphocytes are present in the epidermis in this form, compared with tuberculoid leprosy. Bacilli are absent or rare, but they can be found in dermal nerves and in the arrector pilorum. Nerves are moderately swollen.
In the borderline borderline form of leprosy, diffuse epithelioid granulomas that lack giant cells are observed in the dermis below the subepidermal zone of uninvolved papillary dermis (ie, grenz zone). Nerves are slightly swollen, and acid-fast bacilli are present in moderate numbers.
In the borderline lepromatous form, smaller granulomas with some foamy changes and numerous lymphocytes are observed. Nerves often have an onionskin appearance as a result of invasion of the perineurium. A few epithelioid cells may be observed.
In the lepromatous form of leprosy, a diffuse infiltrate of foamy macrophages is present in the dermis below a subepidermal grenz zone. An enormous number of acid-fast bacilli develop within the foamy macrophages, singly or in clumps, called globi. Lymphocytes are scant, and giant cells are typically absent. Numerous bacilli invade the nerves, but these are fairly well preserved with little infiltrate. Nodular, or dermatofibromalike lesions in lepromatous leprosy, referred to as histoid leprosy, result in a diffuse fascicular arrangement of spindled cells in the dermis admixed with foamy macrophages that contain numerous bacilli.
The histoid form has spindle-shaped clusters of histiocytes in a whorled or parallel pattern. In paucibacillary histoid leprosy, these clusters are in the papillary and mid dermis. Multibacillary histoid leprosy has a grenz zone with the histiocytes located in the mid and deep dermis.33 Globus formation is usually absent. They also tend to grow in an expansive, rather than infiltrative, manner. Bacilli are notably longer than ordinary lepra bacilli.
.
The genomic sequence of M leprae was only completed within the last few years. One important discovery is that although it depends on its host for metabolism, the microorganism retains genes for the formation of a mycobacterial cell wall. Components of the cell wall stimulate a host immunoglobulin M antibody and cell-mediated immune response, while also moderating the bactericidal abilities of macrophages.
The strength of the host's immune system influences the clinical form of the disease. Strong cell-mediated immunity (interferon-gamma, interleukin [IL]–2) and a weak humoral response results in mild forms of disease, with a few well-defined nerves involved and lower bacterial loads. A strong humoral response (IL-4, IL-10) but relatively absent cell-mediated immunity results in lepromatous leprosy, with widespread lesions, extensive skin and nerve involvement, and high bacterial loads. Therefore, a spectrum of disease exists such that cell-mediated immunity dominates in mild forms of leprosy and decreases with increasing clinical severity. Meanwhile, humoral immunity is relatively absent in mild disease and increases with the severity of disease.
Toll-like receptors (TLRs) may also play a role in the pathogenesis of leprosy.2 M leprae activates TLR2 and TLR1, which are found on the surface of Schwann cells, especially with tuberculoid leprosy. Although this cell-mediated immune defense is most active in mild forms of leprosy, it is also likely responsible for the activation of apoptosis genes and, consequently, the hastened onset of nerve damage found in persons with mild disease. Alpha-2 laminin receptors found in the basal lamina of Schwann cells are also a target of entry for M leprae into these cells, while activation of the ErbB2 receptor tyrosine kinase signaling pathway has been identified as a mediator of demyelination in leprosy.3
The activation of macrophages and dendritic cells, both antigen-presenting cells, is involved in the host immune response to M leprae. IL-1beta produced by antigen-presenting cells infected by mycobacteria has been shown to impair the maturation and function of dendritic cells.4 Because bacilli have been found in the endothelium of skin, nervous tissue, and nasal mucosa, endothelial cells are also thought to contribute to the pathogenesis of leprosy. Another pathway exploited by M leprae is the ubiquitin-proteasome pathway, by causing immune cell apoptosis and tumor necrosis factor (TNF)–alpha/IL-10 secretion.5
Other pathways that may be involved are the vitamin D receptor (VDR), transforming growth factor (TGF)–beta, and NOD2-mediated signaling pathways.6,7
A sudden increase in T-cell immunity is responsible for type I reversal reactions. Type II reactions result from activation of TNF-alpha and the deposition of immune complexes in tissues with neutrophilic infiltration and from complement activation in organs. One study found that cyclooxygenase 2 was expressed in microvessels, nerve bundles, and isolated nerve fibers in the dermis and subcutis during reversal reactions.8
Frequency
United States
Approximately 6000 patients with leprosy live in the United States. Approximately 95% of these patients acquired their disease in developing countries. In the United States, 200-300 cases of leprosy are reported each year. States with large immigrant populations (eg, California, New York, Florida) have the largest number of new cases of leprosy. Small endemic foci of leprosy exist in Texas, Louisiana, and Hawaii.
International
The worldwide prevalence of leprosy is reported to be just less than 1 case per 10,000 population. Most affected persons live in the tropics and subtropics. Six major countries in Asia, Africa, and South America have not achieved the goal of elimination (<1 case per 10,000 population). Approximately 86% of reported cases are found in 11 countries: Bangladesh, Brazil, China, Democratic Republic of the Congo, Ethiopia, India, Indonesia, Nepal, Nigeria, Philippines, and the United Republic of Tanzania. Overall, the prevalence of leprosy has decreased since the introduction of short-course MDT in 1982. The global annual detection rate for leprosy has also been declining since 2001.
Mortality/Morbidity
If severe and left untreated, leprosy can cause clinically significant and debilitating deformity. Since 1943, when sulfone was introduced as the first effective treatment for leprosy, antibiotic treatment has dramatically improved patients' outcomes. Early diagnosis and effective antimicrobial treatment can arrest and even cure leprosy.
History
In general, leprosy affects the skin, peripheral nerves, and eyes. Systemic symptoms of leprosy are also possible. Specific symptoms vary with the severity of the disease.
Prodromal symptoms are generally so slight that leprosy is not recognized until a cutaneous eruption is present. However, 90% of patients have a history of numbness first, sometimes years before the skin lesions appear.
Temperature is the first sensation that is lost. Patients cannot sense extremes of hot or cold. The next sensation lost is light touch, then pain, and, finally, deep pressure. These losses are especially apparent in the hands and feet; therefore, the chief complaint may be a burn or ulcer in an anesthetic extremity.
Other parts of the body that might be affected by leprosy are the cool areas, which can include superficial peripheral nerves, the anterior chamber of the eyes, the testes, the chin, malar eminences, earlobes, and knees. From this stage of leprosy, most lesions evolve into the tuberculoid, borderline, or lepromatous types.
Physical
Assess for physical signs of leprosy in 3 general areas: cutaneous lesions, neuropathies, and eyes.
For cutaneous lesions, assess the number and distribution of skin lesions. A hypopigmented macule with a raised border is often the first cutaneous lesion. Plaques are also common. Lesions may or may not be hypoesthetic. Lesions on the buttocks often indicate borderline disease.
Regarding neuropathies, assess for areas of hypoesthesia (light touch, pinprick, temperature and anhidrosis), especially peripheral nerve trunks and cutaneous nerves. The most common nerve affected is the posterior tibial nerve. Others commonly damaged are the ulnar, median, lateral popliteal, and facial nerves. Besides sensory loss, patients may have associated tenderness and motor loss. Nerve palpation, monofilament testing, and voluntary muscle testing are the most useful clinical tests for detecting nerve damage.9
Eye damage is most often seen with facial lesions. Lagophthalmos (inability to close the eye), a late finding in persons with lepromatous leprosy, results from involvement of the zygomatic and temporal branches of the facial nerve (cranial nerve [CN] VII). Involvement of the ophthalmic branch of the trigeminal nerve (CN V) can result in reduced corneal reflex, leaving dry eyes and reduced blinking.
- Clinical tests: Certain tests can be performed in the clinic to aid in the diagnosis of leprosy.
- Tissue smear testing/slit-skin smears: An incision is made in the skin, and the scalpel blade is used to obtain fluid from a lesion. The fluid is placed on a glass slide and stained by using the Ziehl-Neelsen acid-fast method or the Fite method to look for organisms. The bacterial index (BI) is then determined as the number of organisms at 100X with oil immersion. Skin smears have high specificity but low sensitivity because 70% of all patients with leprosy have negative smear results. However, this test is useful because it detects the most infectious patients.
- Histamine testing: This test is used to diagnose postganglionic nerve injury. Histamine diphosphate is dropped on healthy skin and affected skin, and a pinprick is made through each site. The site forms a wheal on healthy skin, but not on skin where nerve damage is present.
- Methacholine sweat testing: An intradermal injection of methacholine demonstrates the absence of sweating in leprous lesions. This test is useful in dark-skinned patients in whom the flare with the histamine test cannot be seen.
- Diagnostic criteria for leprosy10 : The diagnosis of leprosy is primarily a clinical one. In one Ethiopian study, the following criteria had a sensitivity of 97% with a positive predictive value of 98% in diagnosing leprosy. Diagnosis was based on 1 or more of the 3 following signs:
- Hypopigmented or reddish patches with definite loss of sensation
- Thickened peripheral nerves
- Acid-fast bacilli on skin smears or biopsy material
- Classification11 : The Ridley-Jopling classification is used to differentiate types of leprosy and helps in determining the prognosis. Purely neuritic leprosy (asymmetrical peripheral neuropathies with no evident skin lesions), with or without tenosynovitis and symmetric polyarthritis, is also possible.12 A general classification of disease is based on the number of skin lesions present and the number of bacilli found on tissue smears. Paucibacillary disease (indeterminate leprosy and tuberculoid leprosy) has fewer than 5 lesions and no bacilli on smear testing. Five or more lesions with or without bacilli (borderline leprosies and lepromatous leprosy) is considered multibacillary disease.
- Indeterminate leprosy: This early form causes one to a few hypopigmented or, sometimes, erythematous macules. Sensory loss is unusual. Approximately 75% of affected persons have lesions that heal spontaneously. In some, the disease may persist in this indeterminate form. In those with weak immunity, the disease progresses to one of the other forms.
- Tuberculoid leprosy: Skin lesions are few. One erythematous large plaque is usually present, with well-defined borders that are elevated and that slope down into an atrophic center. The lesions can become arciform or annular. They can be found on the face, limbs, or elsewhere, but they spare intertriginous areas and the scalp. Lesions can be dry and scaly, hypohidrotic, and hairless. Another presentation involves a large, asymmetric hypopigmented macule. Both types of lesions are anesthetic and involve alopecia.
- Spontaneous resolution can occur in a few years, leaving pigmentary disturbances or scars. Progression can also occur, leading to borderline-type leprosy. In rare instances in which a patient is untreated for many years, the lepromatous type can develop.
- Neural involvement is common in persons with tuberculoid leprosy; it leads to tender, thickened nerves with subsequent loss of function. The great auricular, common peroneal, ulnar, and radial cutaneous and posterior tibial nerves are often prominent. Nerve damage can happen early, resulting in wrist drop or foot drop.
- Borderline tuberculoid leprosy: Lesions in this form are similar to those in the tuberculoid form, but they are smaller and more numerous. The nerves are less enlarged and alopecia is less in borderline tuberculoid leprosy than in other forms. Disease can remain in this stage, it can convert back to the tuberculoid form, or it can progress to lepromatous leprosy.
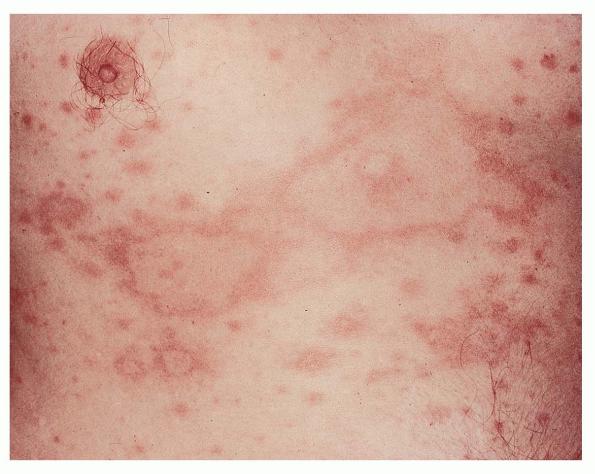
- Borderline borderline leprosy: Cutaneous lesions consist of numerous, red, irregularly shaped plaques that are less well defined than those in the tuberculoid type. Their distribution may mimic those of the lepromatous type, but they are relatively asymmetric. Anesthesia is only moderate. Regional adenopathy may be present. Disease may remain in this stage, it may improve, or it may worsen.
- Borderline lepromatous leprosy: Lesions are numerous and consist of macules, papules, plaques, and nodules. Annular punched-out–appearing lesions that look like inverted saucers are common. Anesthesia is often absent. As with the other forms of borderline leprosy, the disease may remain in this stage, it may improve, or it may regress.
- Lepromatous leprosy: Early cutaneous lesions consist mainly of pale macules. Late infiltrations are present with numerous bacilli. Macular lesions are small, diffuse, and symmetric. The skin may be smooth and shiny, but skin changes do not occur in lepromatous leprosy until late in the course. Therefore, early lepromatous leprosy lesions have little or no loss of sensation, nerves are not thickened, and sweating is normal. Nerve loss is slow and progressive.
- Hypoesthesia occurs first over extensor surfaces of the distal extremities, followed by weakness in the same areas.
- Alopecia affects the lateral aspects of the eyebrows (madarosis), spreading to the eyelashes and then the trunk. Scalp hair remains intact.
- Lepromatous infiltrations can be diffuse, can occur as nodules (called lepromas), or can be plaques. The diffuse type results in the thickened skin appearance of a leonine facies. Neuritic lesions are symmetric and slow to develop.
- Eye involvement occurs, causing pain, photophobia, decreased visual acuity, glaucoma, and blindness.
- Nasal infiltration can cause a saddle-nose deformity and impaired olfaction. Hoarseness ("leprous huskiness") and stridor are a result of laryngeal involvement.13
- Oral lepromas, usually located on the hard and soft palate, uvula, tongue ("cobblestoning"), lips, and gums, can progress to necrosis and ulceration. Tissue destruction may result.14
- Infiltration of the helix or megalobule (elongation and wrinkling of the earlobe) may occur.
- Lymphadenopathy and hepatomegaly can result from organ infiltration.
- Aseptic necrosis and osteomyelitis can occur with repeated trauma after joint invasion.
- Brawny edema of the lower extremities is a late finding.
- Unlike the other types of leprosy, lepromatous leprosy cannot convert back to the less severe borderline or tuberculoid types of disease.
- Histoid leprosy is a recognized clinical variant of lepromatous leprosy.15 It can occur as a result of M leprae resistance to monotherapy of MDT. Reports of de novo histoid leprosy suggest that it may also possibly evolve from borderline or indeterminate leprosy. Paucibacillary and multibacillary forms also exist. They may present as firm plaques or nodules. The lesions may occur on the thighs/buttocks, back, face, and extremities, especially bony areas like the elbows and knees. Eyebrows and nasal cartilage are usually spared.
- Other: Lepra reactions are complications that occur in 50% of patients after the start of therapy or occasionally before therapy (see Complications).
Causes
Leprosy is caused by M leprae, an obligate intracellular, acid-fast, gram-positive bacillus.
- Most persons are immune to leprosy. Subclinical disease is common in endemic areas, and the infection progresses to clinical disease in only a select few.
- Exposure to the nasal discharge of individuals who remain untreated for years is thought to be the main cause of infection. Transmission is not completely understood.
- In addition to exposure to respiratory secretions, exposure to insect vectors and infected soil has been suspected as a possible mode of transmission.
- In endemic countries, household contacts of patients are at increased risk for contracting leprosy. The relative risk is 8-10 times for lepromatous leprosy and 2-4 times for tuberculoid leprosy. In nonendemic countries, household contacts rarely acquire the disease.
- HIV infection is not a risk factor for acquiring leprosy, nor does it increase the clinical symptoms or virulence of leprosy. However, latent cases of leprosy infections may emerge as part of the immune reconstitution inflammatory syndrome after starting highly active antiretroviral therapy.16,17
- One report describes 2 cases of leprosy developing after treatment with infliximab.18 Both patients developed type I reversal reactions after stopping the TNF-alpha inhibitor. Another patient developed a type I reversal reaction after stopping adalimumab therapy, despite no prior diagnosis of leprosy.19
- Several cases of tattoo inoculation leprosy have been reported, most in India.20
- Leprosy has been reported in conjunction with visceral leishmaniasis (kala-azar).
- The following genes have been associated with leprosy; hence, susceptibility to leprosy may be at least partially inheritable7 :
- Susceptible loci have been found on band 10p13 and chromosome 6.
- Associations include HLA-DR2 and HLA-DR3 (tuberculoid disease), as well as HLA-DQ1 (lepromatous leprosy).
- HLA-DRB1*04 is associated with resistance, and HLA-DRB1*10 is associated with susceptibility to leprosy in Brazilian and Vietnamese patients.21
- Genetic variants have been found in the shared promoter region of the PARK2 (parkin) and PACRG genes expressed on monocytes.
- Lymphotoxin-alpha (LTA) + 80 expressed on dendritic cells appears to be a risk factor for early-onset leprosy, independent of PARK2/PARCG and HLA class I and HLA-DRB1 genes.22,23
- Polymorphisms in the gene promoter regions of TNF (multibacillary leprosy) and IL-10 (-819T allele) are noted in leprosy susceptibility.
- Mutations in TLR1 and TLR2 may be involved in susceptibility and/or resistance to other infectious diseases.
- Polymorphisms in the NRAMP1 gene appear on macrophages in multibacillary disease in African patients.
- TaqI polymorphism (tt genotype) at exon 9 of the vitamin D receptor gene is noted
|