













































BLUE NEVUS
Epidemiology
Blue nevi are present in fewer than 1 of 3000 newborns, in approximately 1 of 1000 aged 5 years or less, in 1 percent to 2 percent of white school children, in 3 percent of Japanese adults, and in 0.5 percent to 4.0 percent of healthy white adults. The vast majority of blue nevi are single, small, deep-blue macules or papules approximately 1
to 2 mm in diameter.
BLUE NEVUS AT A GLANCE
· Melanocytic neoplasia comprised of pigmented melanocytic cells in the mid-dermis. Includes common blue, cellular blue, combined blue, atypical, and large patch/plaque lesions.
· Lesions appear as blue, blue-gray, or blue-black papule, nodule, or plaques.
· Lesions are generally acquired but may be congenital.
· Cellular blue nevi may have an elevated risk for development of melanoma.
· Synonyms: benign mesenchymal melanoma, blue neuronevus, chromatophoroma, melanofibroma, Jadassohn-Tièche nevus, and dermal melanocytoma.
· Related lesions include nevus of Ota/Ito and mongolian spot.
Multiple blue nevi may be associated with lentigines, cardiac myxoma, and mucocutaneous myxomas [lentigines, atrial myxomas, mucocutaneous myxomas, and blue (LAMB) nevi, Carney complex]. Blue nevi have been associated with nodular mastocytosis, and a histogenic relationship has been claimed for melanocytes and mast cells.63 Blue nevi have been reported to occur in oral mucosa, uterine cervix, vagina, spermatic cord, prostate, and lymph nodes.64
Etiology and Pathogenesis
The origin of common blue nevi and cellular blue nevi is unknown, but they may be derived from a mutant precursor cell resulting in the accumulation and differentiation of the melanocytic cells in the dermis instead of their normal location in the epidermis. Differentiation towards hair follicular melanocytes is possible. Some varieties of cellular blue nevi stain for CD34,65 suggesting a potential “stem cell” origin. Bednar's tumors (dermatofibrosarcoma protuberans including cells with melanocytic marker expression) also express CD34+ suggesting a similar stem cell origin for these tumors with different differentiation pathways.66 Nevus of Ito/Ota is related to common blue nevi but represents an extensive localized acquired proliferation. The extension of these neoplasms along specific neural pathways may provide insight into the etiology of these dermal proliferations, including the possible role of certain neural factors. Although no specific mutations have been attributed to blue nevi, in the murine system a number of genes have been identified that result in the accumulation of dermal melanocytic cells,67 and it is possible that some of these mutations may be involved in human dermal melanocytoses.
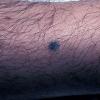
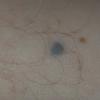
Clinical Findings (Fig. 122-11)
HISTORY
Common blue nevi are usually acquired, and once developed should remain stable. Nevus of Ota and Ito may share similar underlying defects to blue nevi and are also often acquired (in early childhood, often before age 1 year or around puberty) but are far more extensive encompassing a portion of trigeminal (ophthalmic and maxillary) and brachial (posterior supraclavicular and lateral cutaneous) nerve distributions respectively. Dermal melanocytosis (mongolian spot) may also be related to blue nevi, but is usually present at birth or within the first few weeks of life and centered over the lumbosacral area. These lesions usually regress in early childhood but may persist in approximately 10 percent of cases.
CUTANEOUS LESIONS
Common blue nevi are usually solitary, asymptomatic blue, blue-gray, or blue-black papules, usually less than 10 mm in diameter (Fig. 122-12). The blue-gray color of blue nevi is an optical effect of blue light backscatter from the skin over the dermal melanin (Tyndall effect). Hypopigmented, target or targetoid, and combined blue nevi (compound nevomelanocytic nevus and a blue nevus) also exist. Common blue nevi occur anywhere, but about half the reported cases present on the dorsa of hands and feet. Usually, the common blue nevus is singular, but rarely, lesions may be multiple and agminated or arranged in large plaques consisting of multiple solitary papules or nodules with intervening areas of blue discoloration. Common blue nevi also occasionally may have satellite lesions that may be mistaken for melanoma metastasis. Rare giant varieties of congenital blue nevus occur, often with multiple satellite lesions. The large plaque blue nevus (pilar neurocristic hamartoma) may occasionally be associated with a background of lentigo simplex.
The deep penetrating nevus may be considered a unique form of blue nevus, but some would include this lesion in the category of Spitz nevus. Deep penetrating nevi are darkly pigmented, blue-black papules or nodules, mostly on the head and neck or upper extremities, 2 to 9 mm in diameter, and occurring predominantly in the first four decades of life, including childhood
Cellular blue nevi are blue-gray or blue-brown nodules or plaques 1 to 3 cm in diameter, occasionally larger Their surface is usually smooth but may be irregular. Approximately one-half the cases are located on the buttocks or sacrum. Cellular blue nevi may develop in association with CNN, occasionally with target appearance. Cellular blue nevus differs from the common blue nevus in that it is usually larger, more elevated,
more aggressive locally, and occasionally associated with lymph node “benign metastasis.” Complicating the picture is the fact that melanoma may develop in a cellular blue nevus.
Malignant blue nevus (melanoma) may develop in contiguity with a cellular blue nevus, nevus of Ota, combined congenital blue nevus, or de novo. Malignant blue nevus presents as an expanding dermal nodule with or without ulceration. There is some dispute as to whether malignant blue nevus should be considered a separate entity from melanoma or simply referred to as a melanoma developing in a blue nevus.
RELATED PHYSICAL FINDINGS
The presence of epithelioid blue nevi may warrant consideration of Carney complex/myxoma syndrome/LAMB syndrome, with evaluation for related findings, including atrial myxomas and endocrine tumors.
Laboratory Tests
HISTOPATHOLOGY
In common blue nevi, dermal melanocytes appear as melanin-containing fibroblast-like cells grouped in irregular bundles admixed with melanin-containing macrophages, associated with excessive fibrous tissue in the middle or upper reticular dermis, occasionally extending downward to subcutaneous fat or upward to papillary dermis (Fig. 122-13). Elongated melanin-producing dermal melanocytes in common blue nevi usually lie with their long axis parallel to the epidermis. Except in the case of combined blue nevus (with a compound nevomelanocytic nevus component), the epidermis in common blue nevi appears normal. Combined blue nevi have been noted in 1 percent of melanocytic nevi excised for histopathologic examination.70
In cellular blue nevi, there is usually a component of a common blue nevus plus fascicles of spindle-shaped cells with ovoid nuclei and abundant pale cytoplasm with little or no melanin, and often epithelioid cells, present in the dermis and often in subcutaneous fat in nests, bundles, and neuroid forms with little or no intervening stroma (see Fig. 122-13C and D). Epithelioid cell and amelanotic varieties of the cellular blue nevus have been described. Epithelioid blue nevi have been reported in association with cardiac myxoma73 or in isolation.74 Histopathologic diagnosis may be difficult when the common blue nevus component and melanin production are sparse or inapparent. Differentiation of some cellular blue nevi from melanoma can be difficult. Occasionally, small groups of well-differentiated melanocytes are present in the marginal sinus or parenchyma of lymph nodes draining the anatomic site of the cellular blue nevus, making it difficult to differentiate true metastasis from pseudometastasis. It is likely that “inert” deposits of melanocytes in the capsules and peripheral sinuses of lymph nodes draining some varieties of cellular blue nevus are transported passively (see Nodal Nevi).
The malignant blue nevus is a variant of melanoma, distinguished from cellular blue nevus by invasiveness, cellular atypia, pleomorphism, atypical mitoses, and areas of necrosis.
SPECIAL TESTS
Imaging tests of the heart may be required if there is concern for Carney complex/myxoma syndrome/LAMB syndrome.
Differential Diagnosis (Box 122-4)
Complications
A major complication of blue nevi is the potential risk of melanoma. This risk appears to be highest for cellular blue nevi. Melanoma has been noted to evolve in large blue nevus patches or plaques and in associated with nevus of Ota and Ito.
Prognosis and Clinical Course
The natural evolution has not been studied for common blue nevi or cellular blue nevi. It is likely that once established, blue nevi remain unchanged or possibly regress over time. “Change” is worrisome for melanoma development.
Treatment
A common blue nevus that is stable for many years in an adult usually requires no therapy. Sudden appearance of a blue nodule, expansion of a pre-existing blue nodule, a congenital blue nodule, or a relatively large blue nodule or plaque greater than 10 mm in diameter should be considered for histopathologic examination. Excision should include subcutaneous fat to ensure complete removal of deep dermal melanocytes, which are frequently present in the subcutaneous tissue of cellular blue nevus. The large plaque blue nevus (pilar
neurocristic hamartoma) requires consideration for excision or periodic evaluation for suspicious change. Cellular blue nevus should be evaluated for excision because of its malignant potential.
Prevention
The causative factor in eruptive blue nevi has been attributed to sun exposure.75 Thus, as with other nevi, it is reasonable to minimize excessive UVR exposure.
Box 122-4 Differential Diagnosis of Blue Nevus
· Pigmented spindle cell nevus
· Tattoo (traumatic, radiation port marker)
· Primary or metastatic melanoma
· Glomus tumor
· Pyogenic granuloma
· Sclerosing hemangioma
· Dermatofibroma
· Ochronosis




















































