Zoon Balanitis
ETIOLOGY AND PATHOGENESIS
The evidence indicates that ZB is a chronic, reactive, principally irritant mucositis that causes, or is due to, a dysfunctional foreskin. Irritation is induced by retention of urine and squames between two tightly apposed and infrequently and inadequately separated and/or infrequently or inappropriately bathed, commensally hypercolonized, desquamative, secretory epithelial surfaces.
CLINICAL FINDINGS
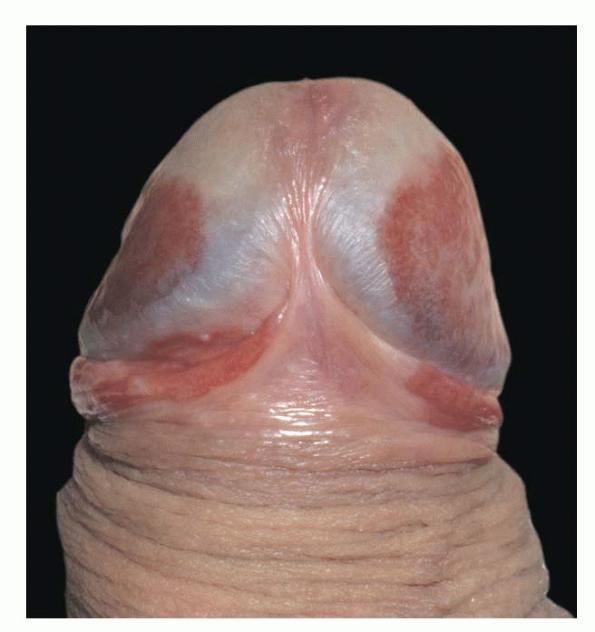
An asymptomatic presentation with little or no dyspareunia is classic. Conversely, the signs can be florid. Well-demarcated, glistening, moist, shiny, bright red or autumn brown patches symmetrically involve the glans and inner prepuce, sparing the keratinized penile shaft or foreskin . Other signs include dark red stippling or “cayenne pepper spots” due to hemosiderin deposition and solitary or multiple lesions of differing sizes (guttate or nummular), characteristically “kissing.” Rarely, erosive and vegetative presentations have been reported, but lesions with asymmetric, atypical, or unusual morphology should be viewed with great suspicion and the organ inspected diligently for other, less florid signs. ZB may be secondary and may thus conceal more subtle evidence of underlying preputial disease such as LSc, pre-cancer, or frank cancer that might have induced the manifest zoonoid changes. Overt cases of other dermatoses such as contact dermatitis, psoriasis, LSc, LP, penis pre-cancer, and penile cancer may appear to have zoonoid changes on clinical and histologic examination . It is possible that some of the clinical and histologic variants that have been reported and the dubious claim that ZB per se is a pre-malignant condition are a consequence of this phenomenon.
ZOON BALANITIS AT A GLANCE
· Zoon plasma cell balanitis (ZB; properly balanoposthitis) affects the middle-aged and older uncircumcised male.
· ZB is a chronic, reactive, irritant mucositis.
· ZB is characterized by silent symptomatology and florid signs.
· Zoonoid inflammation is a common corollary of other dermatoses that cause a dysfunctional prepuce. Asymmetric, atypical, or unusual morphology should be viewed with suspicion.
· Circumcision is the definitive treatment in the majority of cases.
LABORATORY TESTS
On histologic examination the epidermis is attenuated with absence of the granular and horny layers, sparse dyskeratosis and spongiosis, and diamond-or lozenge-shaped basal cell keratinocytes.
In the dermis there are variably seen a band of plasma cells infiltration, extravasated erythrocytes, hemosiderin, fibrosis, and vascular proliferation.
Box 75-5 Differential Diagnosis of Zoon Balanitis
Most Likely
· Psoriasis
· Seborrheic dermatitis
· Lichen sclerosus
· Non-specific balanoposthitis
Consider
· Contact dermatitis
· Erosive lichen planus
· Viral warts
· Herpes simplex
· Fixed drug eruption
Always Rule Out
· Erythroplasia of Queyrat
· Kaposi sarcoma
TREATMENT
Although the condition may be ameliorated by improvement in washing habits and micturition practices and by the intermittent application of mild or potent topical corticosteroids (with or without antibiotics and anticandidals) and topical tacrolimus, ZB usually persists or relapses. Definitive curative treatment is surgical circumcision.