Trichotillomania
Trichotillomania (Greek, hair pulling madness) manifests as a compulsive desire or habit to pull out the hair. It occurs in 0.6 percent to 3.4 percent of adults. In young children, trichotillomania is usually a habit akin to thumb sucking, and most recover spontaneously. In teenagers and adults, though, trichotillomania is a more serious and often intractable psychiatric problem. Childhood trichotillomania is more common in boys, but in the adult form, women outnumber men 7:1. This cause of focal scalp hair loss is classified as an impulse control disorder, and several different underlying psychopathologies can underlie this clinical sign.
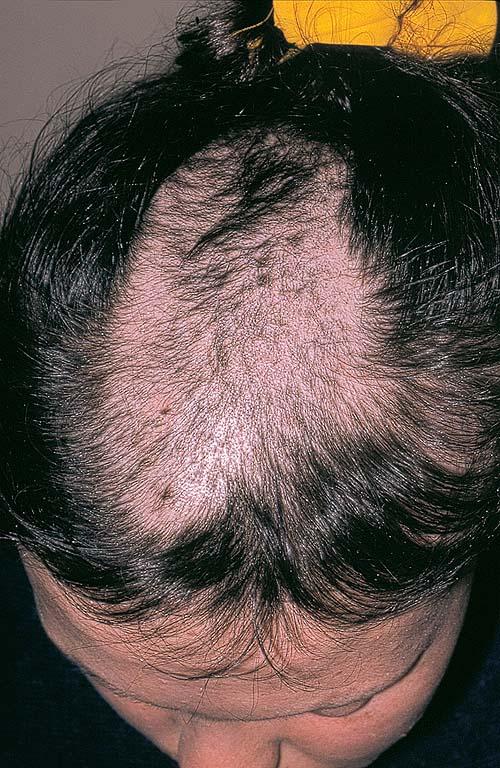
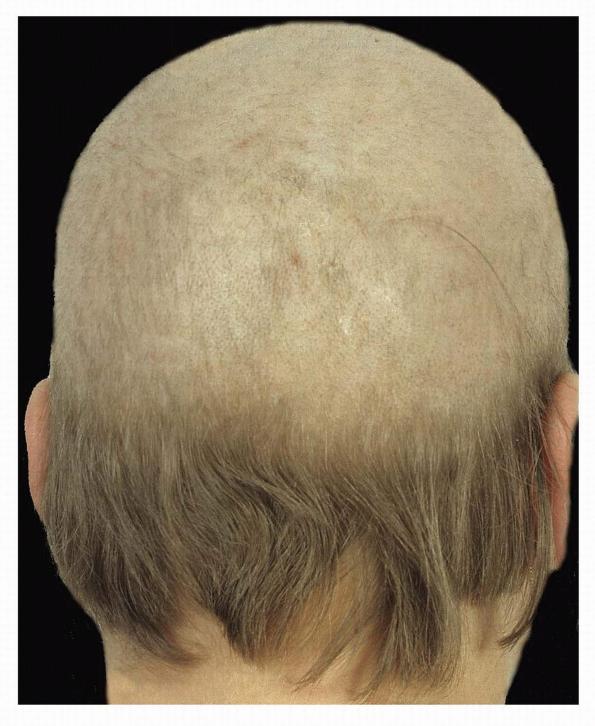
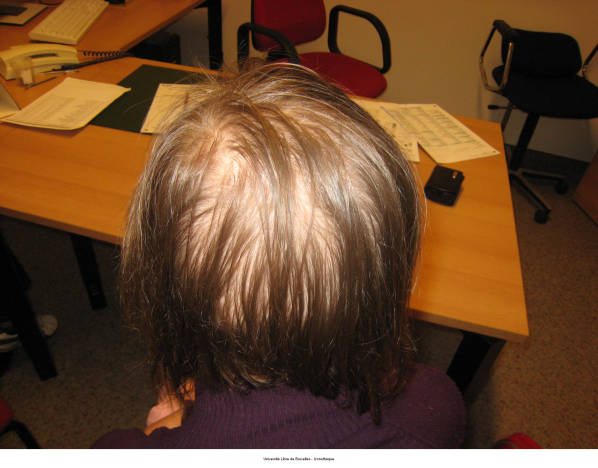
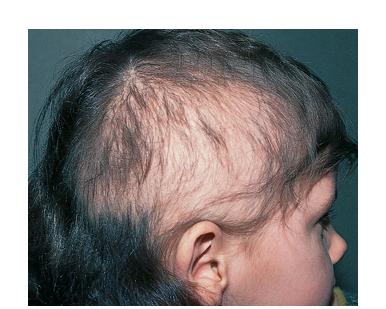
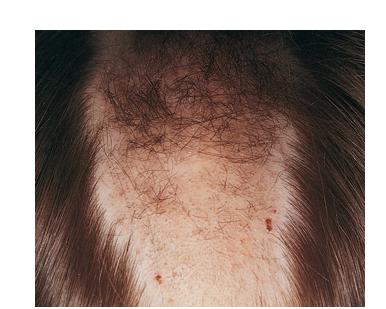
The clinical presentation is usually quite distinctive, with a confluence of very short sparse hairs within an otherwise normal area of the scalp . Microscopic examination of the ends of cut or plucked hairs generally reveals either the tapered tips of newly regrowing anagen hairs or bluntly broken hairs. (A hair pull here is usually negative because the telogen hairs have generally all been dislodged). The most difficult differential diagnosis is from alopecia areata, but the absence of complete hair loss within affected sites and the firmly anchored nature of broken hairs usually permits the distinction to be made. Where doubt remains, a scalp biopsy can be diagnostic, showing the characteristic increase in the number of catagen hairs (rarely seen in biopsies of normal scalp), trichomalacia, and melanin within the follicular canal secondary to traumatic hair removal and the absence or sparsity of a perifollicular inflammatory infiltrate. A vertically oriented hair shaft split, which contains proteinaceous material and erythrocytes (“hamburger sign”) has been proposed as an additional, novel histologic pointer to trichotillomania.
Treatment of these patients is difficult. In children, the habit can often be broken by mere acknowledgement of the problem or behavior modification. Adolescents and adults with this condition present a more challenging problem. In those patients who admit to pulling their hair cognitive behavioral therapy is probably the most effective form of treatment, although there is a high failure rate. Psychotropic drugs, such as clomipramine or sertraline, may also help. The combination of behavioral therapy (habit reversal training) and medication may be more efficacious in the treatment of trichotillomania than either approach alone. Patients who deny the self-inflicted nature of their hair loss usually refuse referral to a psychiatrist or clinical psychologist.