Steatocystoma
Multiplex
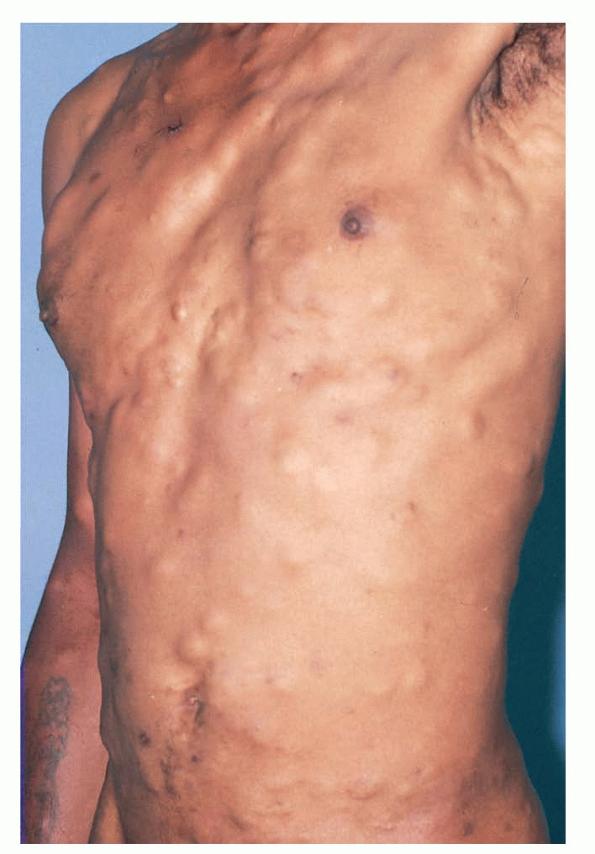
Steatocystoma multiplex are numerous, epithelial-lined, sebum-filled dermal cysts with characteristic sebaceous glands in the cyst walls.
ETIOLOGY AND PATHOGENESIS
Steatocystoma multiplex, (sebocystomatosis, epidermal polycystic disease) can be a sporadic or autosomal-dominant disorder. These lesions can also be found in syndromes
such as Alagille syndrome and pachyonychia congenita type II . In the latter, lesions are associated with mutations in K17. Sporadic solitary lesions are termed steatocystoma simplex.
CLINICAL FEATURES
These lesions present as asymptomatic, yellow or skin-colored dermal papules or cysts located most commonly on the trunk, upper arms, scrotum, or chest . Oily material can be expressed from these lesions when incised. These lesions can become infected and suppurate, resulting in sinus formation and scarring.
PATHOLOGY
The cyst walls of steatocystoma multiplex are composed of stratified, squamous epithelium with an absent granular layer. Sebaceous glands are located in the cyst wall . There is an eosinophilic cuticle on the luminal side of this wall with keratin, oil, and hairs in the lumen.
DIFFERENTIAL DIAGNOSIS
Eruptive vellus hair cysts can mimic steatocystoma multiplex clinically. They may have a tuft of hairs protruding from the cyst centrally, with findings of vellus hairs in the lumen with follicles in the wall. Epidermal inclusion cysts also have to be excluded. The pathogenesis of steatocystoma, epidermal inclusion cysts, and eruptive vellus hair cysts may be similar.
TREATMENT
Removal of these lesions can be successfully achieved with simple excision or drainage of the cyst with manual removal of the cyst wall which, at times, results in the clinical resolution of lesions. Inflamed lesions have been reported to respond to intralesional steroids, carbon dioxide laser, oral retinoids, or cryotherapy.