Sebaceous Carcinoma
EPIDEMIOLOGY
Sebaceous carcinoma occurs more commonly in women than in men, and there may be a history of radiation. Rare cases have been observed in young individuals infected with human immunodeficiency virus.
ETIOLOGY
Sebaceous carcinoma represents a spectrum of rare malignant appendage tumors with sebaceous differentiation that have a potential for aggressive behavior.They have traditionally been divided into ocular and extraocular types. Of these, the ocular type is the most common.
CLINICAL FINDINGS
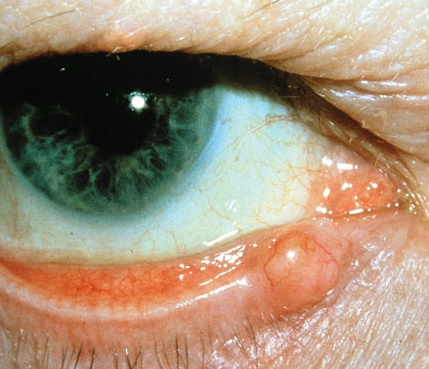
The ocular type of sebaceous carcinoma usually presents in older adults as a small, solitary papule or nodule on the eyelid, particularly around the meibomian glands and glands of Zeiss of the upper eyelid. Lesions are often suspected to be chalazions.
Extraocular sebaceous carcinoma occurs mostly as a yellowish, firm, often ulcerated nodule on the head and neck of elderly individuals. Other anatomic sites, such as the foot and genital regions (labia and penis), may occasionally be involved. Lesions often mimic pyogenic granuloma, hemangioma, or squamous cell carcinoma.
Sebaceous carcinoma represents an important cutaneous marker of Muir-Torre syndrome. In this syndrome, the tumors occur as single or multiple, skin-colored, yellowish or reddish-brown, sometimes ulcerated papules with the appearance of sebaceus hyperplasia and nodules, situated commonly on the face. They may co-exist with keratoacanthomas and/or epidermal cysts. There is still controversy regarding the nature of sebaceous tumors arising in patients with Muir-Torre syndrome. Previous examples have mostly been considered as benign neoplasms (“sebaceous adenomas” or sebaceomas) and less commonly as sebaceous carcinomas. Based mainly on morphology, some authors recently proposed that the vast majority of sebaceous tumors arising in these patients are, in fact, sebaceous carcinomas.
HISTOPATHOLOGY
Sebaceous carcinoma is characterized by an asymmetric lesion centered in the dermis and consisting of variously sized and irregularly shaped aggregations of neoplastic cells. Involvement of the subcutaneous tissue and/or underlying muscle is observed in some cases. Neoplasms may be relatively well-differentiated, with prominent sebaceous lobules and/or sebaceous ductal structures, or show undifferentiated features, with neither readily discernible cytoplasmic vacuoles nor ductal differentiation. The nuclei of the neoplastic cells, especially along the periphery of the tumor nests, tend to be crowded and pleomorphic and may exhibit marked atypia, as well as increased mitotic figures. Sections often reveal areas with geographic necrosis. A peculiar variant with cystic features may be difficult to differentiate from sebaceoma.
Treatment of choice
is surgical excision with adequate margins. Radiation therapy may be effective in some patients with eyelid neoplasms. Up to one-third of patients with the ocular type of sebaceous carcinoma show lymph node metastases, particularly to the preauricular and cervical nodes, and the 5-year mortality rate is about 20 percent. Histopathologic features suggestive of a poor prognosis include the presence of vascular and lymphatic invasion, orbital extension, poor differentiation, an infiltrative growth pattern, and large tumor size. In contrast to ocular tumors, extraocular sebaceous carcinoma very rarely reveals nodal or visceral metastases. Sebaceous carcinomas arising in Muir-Torre syndrome, like visceral malignancies in these patients, also seem to be less aggressive than their ocular counterpart, which is unassociated with the syndrome