Scarlet Fever
Scarlet fever is a syndrome characterized by exudative pharyngitis, fever, and scarlatiniform rash. It is most commonly due to pyrogenic exotoxin-producing group A streptococcus, although staphylococcal infections can produce a similar-appearing disease. The exact mechanism by which toxins produce the symptom complex is unclear. Compelling studies by Schlievert demonstrated that the scarlatiniform eruption could only be induced in mice that were previously sensitized against toxins. This suggests that a combination of conventional delayed type and superantigen-mediated processes are occurring. It should be noted that streptococcal toxins, especially SPEA, have areas of significant homology with collagen, which could provide a mechanism for rare autoimmune sequelae of streptococcal scarlet fever, including renal failure and rheumatic fever. Scarlet fever is no longer the major public health threat it was in the past because of antibiotic treatment and because most streptococcal isolates causing scarlet fever express the less virulent SPEB and SPEC rather than SPEA.
CLINICAL FINDINGS
Streptococcal Scarlet Fever.
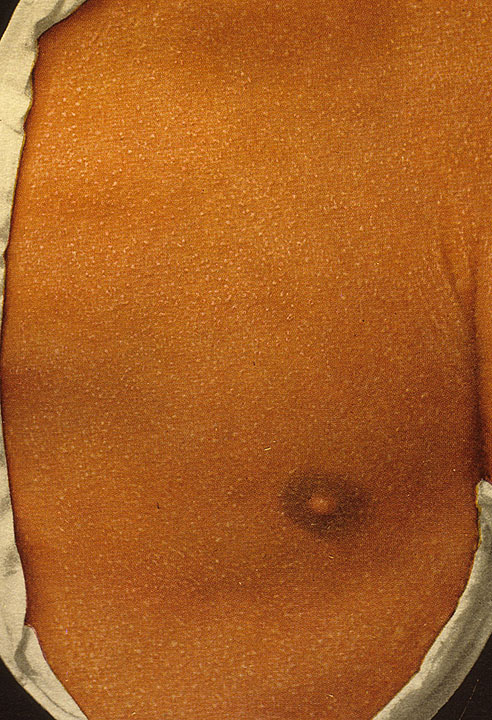
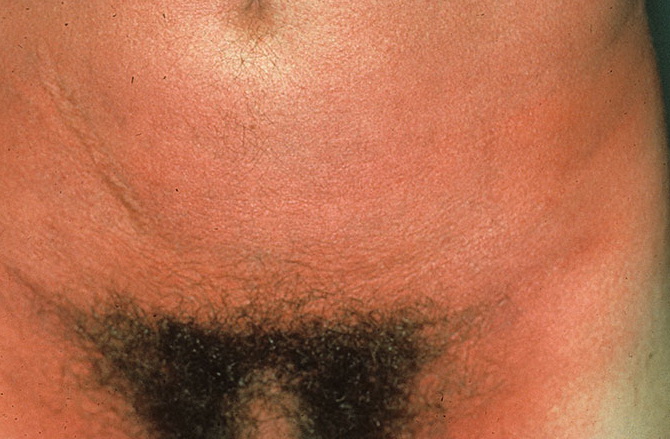
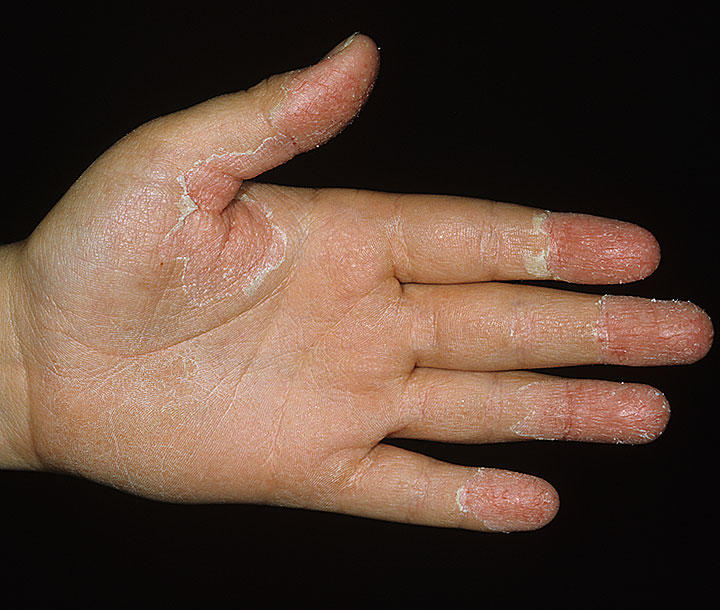
Streptococcal scarlet fever is a childhood disease that occurs most commonly in winter and early spring. It is estimated that up to 10 percent of childhood group A streptococcal pharyngitis patients develop scarlet fever. Approximately 12 hours to 5 days after exposure, an abrupt prodrome consisting of pharyngitis, headache, vomiting, abdominal pain, and fever develops. The rash appears 1 to 2 days after onset of the illness, first on the neck and then extending to the trunk and extremities, although it spares the palms and soles. The exanthem texture is usually coarse, like fine-grade sandpaper, and the erythema blanches with pressure . The skin can be mildly pruritic but usually is not painful. A few days after generalization of the exanthem, the rash becomes more intense around skin folds and lines of confluent petechiae, due to increased capillary fragility (Pastia's sign), can be seen. The generalized exanthem begins to fade 3 to 4 days after onset and a desquamative phase begins, usually starting on the face. Peeling from the palms and fingers and, sometimes, soles occurs approximately 1 week later and can last for up to 1 month .
Oral findings of streptococcal scarlet fever include edematous, erythematous tonsils sometimes covered with a yellow, gray, or white exudate. Tender anterior cervical lymphadenopathy is
common. Petechiae and punctate red macules are seen on the soft palate and uvula (Forschheimer's spots). A flushed face with circumoral pallor is also commonly noted . In scarlet fever, the tongue demonstrates characteristic changes. During the first 2 days of the disease, the tongue has a white coat through which the red and edematous papillae project (white strawberry tongue). After 2 days, desquamation occurs, resulting in a red tongue with prominent papillae (red strawberry tongue) .
The diagnosis of scarlet fever is made by the characteristic clinical signs and confirmed by the rapid streptococcal test or throat culture. Scarlet fever usually follows a benign course, and any undue morbidity or mortality is likely due to suppurative complications, including peritonsillar abscess, sinusitis, pneumonia, and meningitis or non-suppurative complications associated with immune-related rheumatic fever or glomerulonephritis. The risk of acute rheumatic fever following an untreated group A streptococcal infection has been estimated to be approximately 3 percent in epidemics and 0.3 percent in endemic circumstances. Glomerulonephritis can occur in up to 10 percent to 15 percent after infection with nephritogenic group A streptococcal strain. In addition to pharyngitis, group A streptococcus can cause scarlet-fever-like eruptions from skin (often surgical wounds) or uterine infections.
Scarlet fever is treated by antibiotics (penicillin or erythromycin for a 10-day course) and supportive care. Fever usually abates within 12 to 24 hours after initiation of antibiotic therapy. Recurrences are common.
Staphylococcal Scarlet Fever.
Staphylococcal scarlet fever, also known as scarlatiniform erythroderma or rash, was first described almost 90 years ago and, until recently, was considered to be a milder or abortive form of SSSS. Patients usually develop a generalized erythroderma with a roughened, sandpaper-like texture very much like in streptococcal scarlet fever. However, the exanthem of staphylococcal scarlet fever tends to be more tender than corresponding streptococcal scarlet fever. Systemic signs including malaise and fever are invariably present. Within a few days of initiation of the rash, thick flakes develop, and the entire skin desquamates over the subsequent week. Unlike generalized SSSS, the scarlatiniform eruption is not associated with the formation of bullae or superficial exfoliation and can be very difficult to differentiate from other infectious erythrodermal causes such as TSS and streptococcal scarlet fever. Scarlet fever induced by staphylococci differs from streptococcalmediated disease by the lack of pharyngitis. A recent study by Wang and colleagues examined the clinical characteristics and toxin detected in 20 children with staphylococcal scarlet fever. They found that all of the patient's staphylococcal infections arose from the skin; 16 of 20 cases from furuncles/carbuncles; two each from abscesses or wound infections. All of the S. aureus strains expressed SEB. Of note, SEB shows significant protein sequence homology with SPEA, a known exotoxin associated with streptococcal scarlet fever. Yet other studies have implicated other staphylococcal enterotoxins. One explanation for this heterogeneity of toxins associated with this disorder is that the diagnosis is made upon clinical grounds. It is indeed possible that staphylococcal scarlet fever represents an incomplete form of TSS, in which toxins spread from the skin, thus activating the skin-associated lymphoid tissue rather than mucosal-associated lymphoid tissue. Because most cases of streptococcal scarlet fever arise from a pharyngitis, the lack of a pharyngitis in a patient with characteristic rash and other clinical signs of scarlet fever should alert the clinician to look for a localized nidus of infection (e.g., furuncle) that could be cultured to establish the diagnosis.
DIFFERENTIAL DIAGNOSIS
The diagnosis of scarlet fever is made on clinical grounds with supporting positive bacterial cultures. The differential diagnosis should include other toxin-mediated disorders including SSSS. Although Kawasaki syndrome (see Chap. 168) has many similar clinical findings including mucosal involvement (e.g., strawberry tongue), swelling of extremities, and desquamation of palms and soles during convalescence, Kawasaki syndrome differs in that the course of fever is prolonged and cultures would be expected to be negative. Atypical drug hypersensitivity reactions can have some cutaneous features, but would lack the mucosal signs. There is usually a history of offending drug and peripheral eosinophilia. Scarlet fever from group A streptococcus can usually be differentiated from that induced by S. aureus as the usual nidus of infection in streptococcal scarlet fever is from a pharyngitis while the staphylococcal variant usually has its infectious nidus in the skin.
TREATMENT AND PROGNOSIS
The treatment of scarlet fever includes antibiotics to eradicate the offending bacteria. If the localized nidus of infection is an abscess or furuncle/carbuncle, it should be drained. Acute rheumatic fever or glomerulonephritis is not associated with staphylococcal scarlet fever. For situations in which more systemic signs resemble TSS, the treatment should be that of TSS.