






















Reactive perforating collagenosis
Reactive perforating collagenosis is a rare skin disorder characterized by the transepidermal elimination of altered collagen through the epidermis. The 2 distinct forms of are an inherited form that manifests in childhood and an acquired sporadic form that occurs in adulthood.
The 4 primary perforating diseases are reactive perforating collagenosis, elastosis perforans serpiginosum, Kyrle disease, and perforating folliculitis, although whether perforating folliculitis is a primary perforating disease has been questioned, given that ruptured follicles are a feature of many infective conditions.
Some authors reserve the term reactive perforating collagenosis for the rare inherited form of the disease, preferring the term acquired perforating dermatosis for the acquired form. This article describes both inherited reactive perforating collagenosis and acquired reactive perforating collagenosis.
The major abnormality in reactive perforating collagenosis is focal damage to collagen and the elimination of the disrupted collagen through the epidermis.1 A frequent association with pruritus, the tendency to the Koebner phenomenon and the distribution of lesions on trauma-prone areas provides evidence that superficial trauma (eg, scratching) may play a part in the etiology of reactive perforating collagenosis. Cold may precipitate the lesions, especially in the inherited form.
The acquired form usually occurs in patients with diabetes or chronic renal failure, especially those receiving dialysis. Other associations with systemic diseases, such as malignancy, have been reported.
Faver et al has proposed diagnostic criteria for the adult (acquired) form of reactive perforating collagenosis, as follows2 :
- Elimination of necrotic basophilic collagen bundles into a cup-shaped epidermal depression as seen in biopsy specimens
- Umbilicated papules or nodules with a central, adherent keratotic plug
- Onset of lesions after age 18 years
- Small, keratotic papules develop after minor trauma. The lesions start as pin-sized lesions, and they grow into larger papules/nodules over a few weeks. They heal with minor scarring.
- Intense pruritus is a feature of the acquired form of reactive perforating collagenosis. Many patients have diabetes or renal failure, and many will be on hemodialysis.
- A positive family history may be elicited in the childhood form of reactive perforating collagenosis.
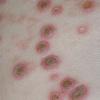
- Skin lesions of reactive perforating collagenosis
- Flesh-colored, umbilicated, dome-shaped papules or nodules as large as 10 mm in diameter are typical. They have an adherent, keratinous plug. A giant variant of reactive perforating collagenosis has been described.5
- Reactive perforating collagenosis lesions may occur in a linear configuration, exhibiting the Koebner phenomenon.
- Residual scarring may be seen from previously healed lesions.
Skin distribution of reactive perforating collagenosis
- Lesions are most commonly found on the extensor surfaces of the limbs and the dorsa of the hands.
- Reactive perforating collagenosis lesions may also occur on the trunk and the face.
The childhood form of reactive perforating collagenosis is inherited.6 A number of affected families have been reported. The mode of inheritance is not clear. Reports of affected families reveal autosomal dominant inheritance, autosomal recessive inheritance, and sporadic cases.
- The underlying cause of reactive perforating collagenosis is unknown, but an abnormal response to superficial trauma (eg, scratching) may be involved. Papules have been reported following scratches, acne spots, insect bites,7 and scabies.8 Lesions of reactive perforating collagenosis have been experimentally induced in susceptible skin by scratching.9
- The acquired form of reactive perforating collagenosis may occur in association with chronic renal failure, often in a patient with underlying diabetes. In both the United Kingdom and the United States, the prevalence of this disorder in patients on dialysis is approximately 10%.3,4
- The acquired form of reactive perforating collagenosis also can occur in association with other nephropathies without diabetes.
- Acquired reactive perforating collagenosis has been reported in association with hypothyroidism, hyperparathyroidism, and liver dysfunction.2
- Malignancies, including lymphoma, hepatocellular carcinoma,10 periampullary carcinoma,11 and thyroid cancer,12 have been associated with the acquired form of reactive perforating collagenosis.
- Indinavir has induced reactive perforating dermatosis in 2 patients with HIV disease.1
- The purpose of any investigation is to search for underlying causes, particularly causes of pruritus.
- Urea and creatinine determinations are needed to detect any underlying renal impairment. A creatinine clearance test and other more complex renal investigations may be required.
- Ferritin levels and a full blood cell count can help detect anemia. Low iron stores can cause pruritus.
- Random glucose testing can help detect diabetes.
- Skin biopsy is essential to make a diagnosis.
Histologic Findings
The histology varies with the stage of the reactive perforating collagenosis. Early lesions show epidermal hyperplasia associated with underlying degenerate basophilic collagen fibers. In established lesions, a cup-shaped depression of the epidermis associated with a keratin plug containing parakeratosis, inflammatory debris and collagen fibers can be seen.
Vertically orientated basophilic collagen fibers are seen in the underlying dermis, with focal extrusion through the epidermis
The epidermis is atrophic and may show ulceration. However, at the edges of the cup-shaped invagination, the epidermis is hyperplastic. Additionally, a mild perivascular lymphohistiocytic infiltrate can be seen.
Extruded collagen fibers may be demonstrated with elastic van Gieson (EVG) staining, which stains the fibers red. No extrusion of elastic fibers should be seen (staining black with EVG).
Medical Care
Treatment of reactive perforating collagenosis lesions is often unsatisfactory; in many cases, the lesions are self-healing, but usually are recurrent.
- Anecdotal reports describe successful therapy for reactive perforating collagenosis with retinoids,14 allopurinol,5 doxycycline,15 UVB,16 and psoralen ultraviolet light A.17 Phototherapy is a good choice for patients with coexistent renal disease and associated pruritus.
- Topical steroids are usually not helpful, but intralesional steroids have been successful.7
- Emollients and systemic antihistamines seem helpful in controlling pruritus.
- The inherited form of reactive perforating collagenosis is not associated with any systemic complications.
- The acquired form of reactive perforating collagenosis occurs in patients with multiple medical problems, but whether the development of the lesions implies a poorer prognosis is unclear.
























