|
Polymorphous light eruption= الاندفاع الضيائي متعدد الاشكال |
 |
 |
 |
|
Polymorphic Light Eruption
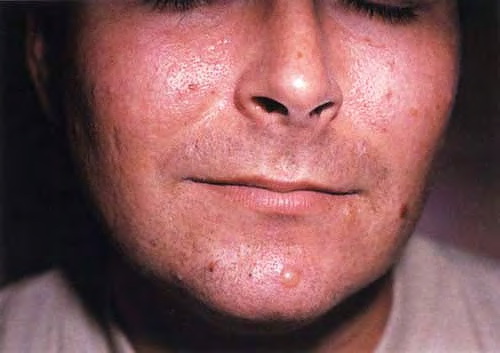
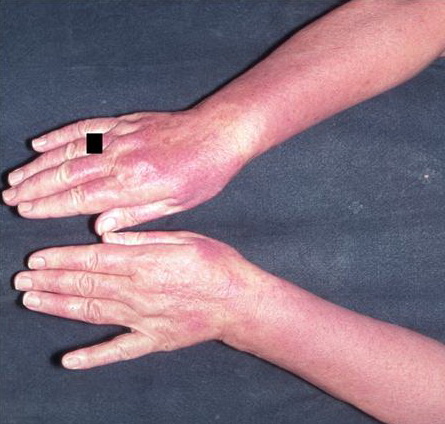
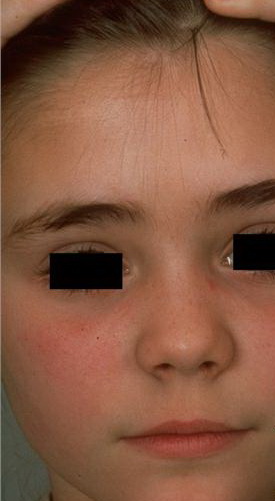
PMLE is a commonly occurring, transient, intermittent, approximately symmetrical UVR-induced eruption of nonscarring, erythematous, itchy papules, plaques, or vesicles of usually only some exposed skin that
is most severe during spring, summer, and sunny vacations and most common in young women . It is seen most frequently at temperate latitudes, affecting up to one in five subjects of any skin coloring, with attacks following around 15 minutes to a few hours of sun exposure, or occasionally a few days after a period with little exposure such as on vacation, and lasting for hours, days, or rarely weeks before often recurring, sometimes with gradual reduction in severity, from spring until fall. Some but usually not all exposed skin is affected, usually symmetrically, with normally uncovered sites most frequently being spared. Diagnosis is made from the history and clinical findings in the presence of normal circulating antinuclear factor and extractable nuclear antibody titers and of normal urinary, stool, and blood porphyrin concentrations. However, if there is diagnostic uncertainty, lesional histology is generally very helpful, while broad-spectrum or monochromatic skin irradiation may respectively induce the typical eruption or abnormal erythemal or papular responses. Treatment, either prophylactic or remedial, is for the most part effective. Often, the restriction of UVR exposure, use of appropriate clothing, and regular application of high-protection, broad-spectrum sunscreens during exposure are satisfactory for mild disease. In more severe instances, prior to the beginning of summer, four to six weekly courses of broadband or, more commonly, low-dose narrowband (311-312 nm) ultraviolet B (UVB) phototherapy, or slightly more reliably, low-dose psoralen photochemotherapy (PUVA), are usually effective. If an eruption should develop despite these measures, a short course of systemic steroid therapy usually abolishes it quickly. Azathioprine and cyclosporine have rarely been used effectively for very severe disease. The value of other previously advocated medications, such as antimalarials and beta-carotene, has not been confirmed in controlled trials.
|
|
Histopathology
The histologic findings vary according to the age of the lesion sampled. Very early lesions show either a normal epidermis or mild spongiosis with focal lymphocyte exocytosis and an underlying mild or occasionally moderate, superficial and deep, perivascular and periadnexal, lymphohistiocytic inflammatory cell infiltrate the lymphocytes have a T-helper phenotype (CD3/CD4 positive). Interestingly, in experimentally induced PMLE lesions, the infiltrate in the first 72 hours postinduction also has a predominant T-helper phenotype but thereafter a mainly T-cytotoxic type (CD3/CD8 positive) . Occasional eosinophils and rare neutrophils may also be found. As lesions progress, there is marked edema of the papillary dermis and more prominent dermal inflammation
in such cases, the histologic picture may resemble cutaneous lupus erythematosus (see next section). Exceptionally, a fairly prominent dermal infiltrate may raise the possibility of lymphoma. In a few cases, the histologic findings may be minimal despite the presence of prominent clinical changes .
Pathogenesis. The eruption of PMLE is induced by exposure to UVR, particularly from strong summer sunlight (2,3). Artificial reproduction is less easy, and exact action spectra have not been conclusively determined. Nevertheless, broadly speaking, the responsible wavelengths appear to be UVB in around half of patients and ultraviolet A (UVA) in three quarters, which includes both in one quarter, while visible light has also rarely been incriminated. The eruption itself appears very likely to be a DTH response in view of its pattern of dermal cellular infiltration, cytokine production, and adhesion molecule expression, arguably to UVR-induced, endogenous, cutaneous autoantigen. Further, it appears that a genetically determined impairment of the normal UVR-induced suppression of
induction, but interestingly not elicitation, of DTH reactions in the skin is responsible
.
Differential Diagnosis.
The diagnosis is generally apparent from the clinical history, in which sun exposure is nearly always clearly incriminated in causing the typical eruption, provided that the circulating antinuclear and extractable nuclear antibody titers and urinary, stool, and blood porphyrin concentrations are normal. Histologically, PMLE must be differentiated from lupus erythematosus, the porphyrias, AP, Jessner's lymphocytic infiltrate, cutaneous T-cell lymphoma, chilblains, and rosacea . In cutaneous lupus erythematosus, the interface change is more prominent not only in the epidermis but also in adnexal structures, apoptotic keratinocytes are often seen, and papillary dermal edema is not a feature. In addition, dermal mucin deposition may be seen in lupus and is absent in PMLE. AP usually displays changes secondary to excoriation, variable epidermal hyperplasia, and more prominent lymphocyte spongiosis and exocytosis; however, early lesions in both conditions may show very similar microscopic findings, except that dermal edema is usually absent in AP. In Jessner's lymphocytic infiltrate, epidermal changes are absent, there is no papillary dermal edema, and the dermal mononuclear cell infiltrate tends to be more prominent. Cutaneous T-cell lymphoma is only rarely included in the differential diagnosis of PMLE, mainly when the dermal infiltrate is prominent; however, the exocytosis of lymphocytes with irregular nuclear outlines is not a feature of the latter, which usually also shows variable spongiosis. The histology of chilblains is almost identical to that of PMLE, particularly when there is prominent papillary dermal edema, but fortunately the clinical setting of each disease usually allows distinction. Rosacea shows no epidermal change, dermal edema is absent, the dermal infiltrate is mild and surrounds superficial small blood vessels and adnexal structures, and focal lymphocytic exocytosis into hair follicles is often seen.
|
|
|
|
|