| Pityriasis alba =النخالية البيضاء او القاصرة اللون |
|
|
Pityriasis Alba
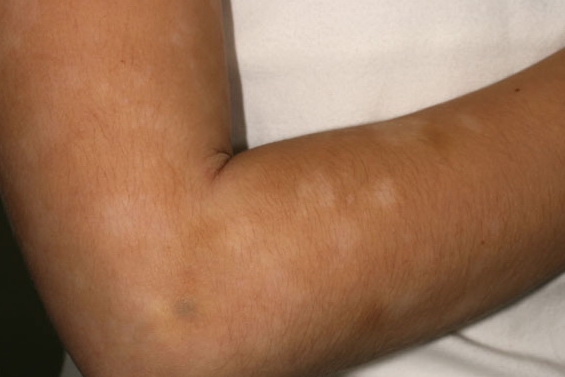
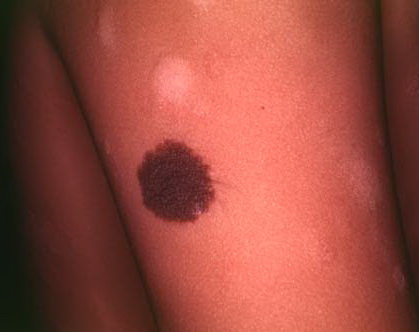
BackgroundPityriasis alba is a nonspecific dermatitis of unknown etiology that causes erythematous scaly patches. These resolve and leave areas of hypopigmentation that slowly repigment to normal. Pityriasis alba commonly occurs in children. PathophysiologyPityriasis alba has been regarded as a manifestation of atopic dermatitis.1,2 Pityriasis alba is known to occur in nonatopic individuals. Pityriacitrin, a substance produced by Malassezia yeasts, acts as a natural sunscreen, but much of the hypopigmentation results from a failure of melanin transfer from melanocytes to keratinocytes.3 FrequencyThe frequency of pityriasis alba both in the United States and internationally is unknown. InternationalA large study in a tropical region in schoolchildren showed that the prevalence of pityriasis alba was 9.9%. Another study in Nepal showed that the prevalence of pityriasis alba within a wide range of dermatoses was 5.2%.4 Mortality/MorbidityPityriasis alba is not associated with mortality. Pityriasis alba is usually a self-limited, asymptomatic disease. RacePityriasis alba can affect persons of any race, but it may be more prominent and cosmetically more troublesome in dark-skinned patients.5 SexBoth sexes are equally susceptible to pityriasis alba, but it is thought that males are affected more frequently.6 AgePityriasis alba occurs predominantly in children aged 3-16 years.5 but can occur in adults.7 ClinicalHistory
Physical
Causes
Reported contributory factors related to the development of pityriasis alba are excessive and unprotected sun exposure, poor hygienic habits, and environmental influences such as temperature, humidity, and altitude TreatmentMedical CarePityriasis alba resolves spontaneously and may not require treatment.
ConsultationsA dermatologist may be consulted for cosmetic camouflage. DietNo dietary recommendations are currently proposed. ActivityNo specific activity limitations or exercises are recommended. Photoprotection may be considered. Also see Sunscreens and Photoprotection. MedicationResponse to treatment for pityriasis alba often is disappointing. EmollientsA variety of lotions, creams, and ointments that contain hydrocarbons, oil, waxes, and long-chain fatty acids aid in retaining moisture in the skin especially if applied immediately after bathing. A bland emollient may be used to reduce the scaling.
Aqueous cream (Curel, Cetaphil, Nivea, Lubriderm)Oil in water emulsion that spreads easily and helps retain moisture in the skin. AdultApply 2-6 times/d PediatricAdminister as in adults None reported Documented hypersensitivity PregnancyA - Fetal risk not revealed in controlled studies in humans PrecautionsNone reported Corticosteroids, topicalReducing inflammation helps reduce symptoms and helps resolve lesions.
Hydrocortisone (Cortaid, Dermacort)1% or 2.5% hydrocortisone cream or ointment. Adrenocorticosteroid derivative suitable for application to skin or external mucous membranes. Has mineralocorticoid and glucocorticoid effects resulting in anti-inflammatory activity. AdultApply to face bid for 1 wk or until lesion improves PediatricApply as in adults None reported Documented hypersensitivity; viral, fungal, and bacterial skin infections PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsProlonged use, applying over large surface areas, application of potent steroids, and occlusive dressings may increase systemic absorption of corticosteroids and may cause Cushing syndrome, reversible HPA axis suppression, hyperglycemia, and glycosuria Immunosuppressant Agent
Tacrolimus (Protopic)Mechanism of action in atopic dermatitis not known. Reduces itching and inflammation by suppressing the release of cytokines from T cells. Also inhibits transcription for genes that encode IL-3, IL-4, IL-5, GM-CSF, and TNF-alpha, all of which are involved in early stages of T-cell activation. Additionally, may inhibit release of preformed mediators from skin mast cells and basophils and down-regulate expression of FCeRI on Langerhans cells. Can be used in patients as young as 2 y. Drugs of this class are more expensive than topical corticosteroids. Available as ointment in concentrations of 0.03 and 0.1%. Indicated only after other treatment options have failed. AdultApply thin layer to affected skin areas bid and rub in gently and completely; continue treatment for 1 wk after clearing of signs and symptoms Pediatric<2 years: Not recommended None reported Documented hypersensitivity to tacrolimus or components of ointment PregnancyC - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus PrecautionsPatients may experience a burning sensation during first few days of application; skin can become photosensitive and patients should be cautioned about exposure to direct or artificial sunlight and to use sunscreen; safety and efficacy in infected atopic dermatitis is not known; application under occlusion, which may promote systemic exposure, has not been evaluated (do not use ointment with occlusive dressings); absorption following topical applications of ointment is minimal (relative to systemic administration), but is excreted in human milk and, thus, a decision should be made whether to discontinue nursing or to discontinue drug, taking into account importance of drug to mother (potential for serious adverse reactions in nursing infants from tacrolimus should also be a concern); caution with conditions that suppress the immune system (eg, AIDS, cancer) ; possible risk of lymph node or skin cancer based on animal studies and a small number of patients; may increase risk of viral infections; other adverse effects include headache, sore throat, flulike symptoms, fever, and cough
|