PINTA (CARATE, MAL DE PINTA, AZUL)
Epidemiology and Etiology
Pinta (“colored spot” in Spanish) is caused by T. carateum, named after the Colombian word for the disease (carate). The organism can be propagated only in primates, and no isolates are known to exist.
The disease affects predominantly poor, undernourished infants, children, and adolescents who live in small, remote, crowded villages in hot, semiarid coastal areas. Twenty years ago, approximately 750,000 cases were estimated, but now only a few hundred new cases are reported each year, mainly in southern Mexico, Brazil, Colombia, Venezuela, Peru, and Ecuador.
Transmission occurs from repeated, direct contact of the exposed skin of a healthy person with a cutaneous or mucous membrane lesion on an infected person.
Pinta is the only treponematosis with clinical manifestations confined to the skin. As in syphilis, there are three distinct clinical stages. Lesions at different stages may be present in a single patient. Because cell-mediated immunity is not completely effective against the organism, the infection persists indefinitely, and people of all ages can be infected. However, half of all patients are younger than 15 years of age.
Primary Stage
After an incubation period of 15 to 30 days, one to three erythematous papules develop at the site(s) of inoculation. These primary lesions may be pruritic and over weeks to months enlarge or coalesce with other lesions to achieve a size of 1 to 3 cm. The resulting plaques are irregular, scaly, lichenified, and centrally paler, and can grow to a diameter of 20 cm Over time, the centers become hypochromic, grayish, light blue, or pale mauve. Primary lesions usually develop in exposed areas, especially the hands, feet, arms, legs, face, and neck. They can persist for years and eventually heal spontaneously with residual dyspigmentation. Regional lymph nodes may become enlarged.
Secondary Stage
Secondary lesions (pintids) usually arise 1 to 12 months, but sometimes years, after the appearance of the primary lesions. They may encircle the sites of the primary lesions or erupt generally on the body. Pintids may occur on the palms, soles, and groin. Secondary lesions may be indistinguishable from primary lesions but are smaller, usually asymptomatic, and psoriasiform. Some lesions may be circinate or annular with raised borders where the number of treponemes is highest. Gradually, the lesions turn brown or copper colored and eventually slate blue, gray, or black. More than one color may be present within a plaque. Lesions can occur up to 10 years after the initial infection.
Tertiary Stage
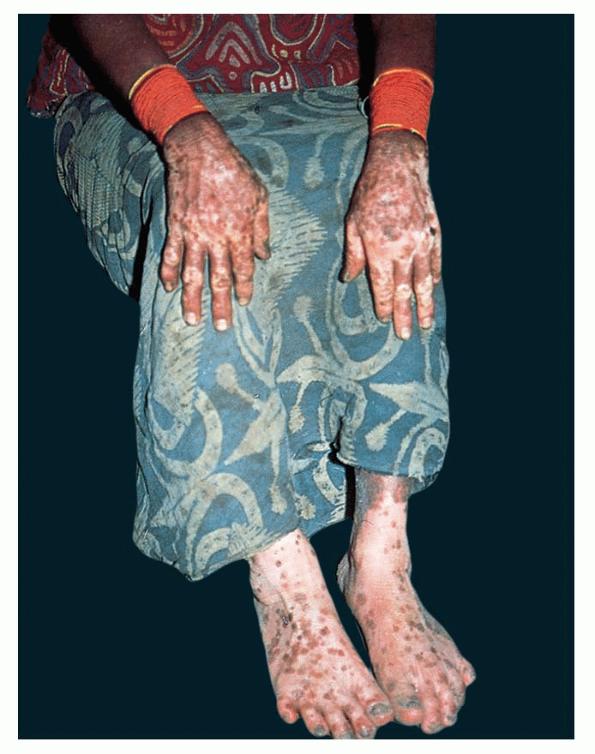
Late lesions usually develop between 2 and 4 years after the onset of the disease and 3 months to 10 years after the appearance of the secondary-stage lesions. Typically, patients have dyschromic patches that are hyperchromic, hypochromic, and achromic, which impart a mottled pattern with a variegated palette of white, brown, blue, red, and violet. The lesions have irregular borders and vary in size. The more commonly involved areas are the wrists, palms, ankles, and elbows as well as the skin around and within old lesions . In such areas, the lesions appear scarred and atrophic (cicatricial lesions of pinta). Lymphadenopathy may develop during any stage of pinta. Patients with only late-stage lesions may appear to have vitiligo (vitiligo of pinta).