




PILOMATRICOMA
Epidemiology.
Pilomatricoma most commonly occurs in children and young persons.Some tumors arise in older adults. Mutation of the β-catenin gene, a mediator in the Wnt signal transduction pathway, is common in pilomatricomas.
Etiology.
Pilomatricoma (calcifying epithelioma of Malherbe) is a relatively common appendage tumor that predominantly shows differentiation toward the matrical portion of a normal hair follicle at the level of the bulb.
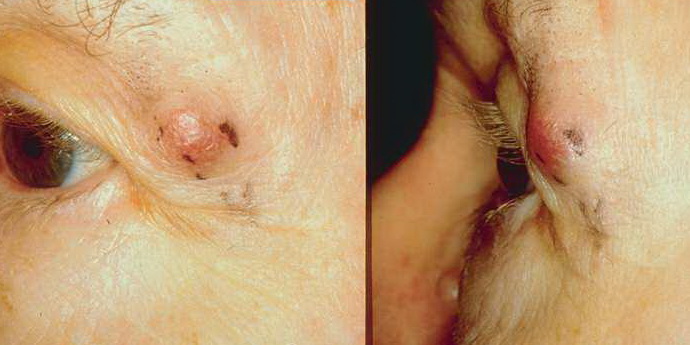
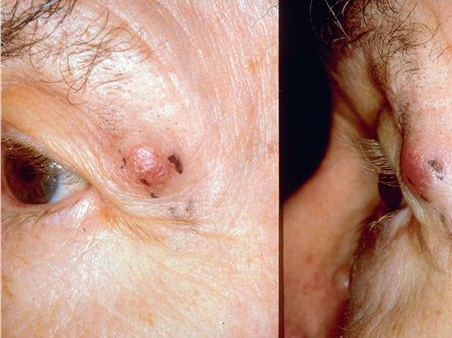
Clinical Findings.
Lesions present as solitary, skin-colored, or pigmented cystic or firm nodules on the head and neck and upper extremities. Unusual clinical features include rapidly growing tumors, lesions associated with overlying striae or anetodermic changes, and tumor arising in a nevus sebaceus. Several variants, including multiple pilomatricomas, bullous or giant tumors, and lymphangiectatic variants, have been reported. Multiple pilomatricomas have also been reported in patients with Gardner syndrome.
Histopathology.
Pilomatricoma shows a spectrum of morphologic features that mainly reflect different evolutionary stages. Early and well-developed pilomatricomas reveal variably sized, round to oval cystic lesions lined by a basaloid epithelium at the periphery and filled in the center with masses of eosinophilic, faulty hair matrix material containing “shadow” (“ghost”) cells
Basaloid (matrical) cells show monomorphous round nuclei with one or more distinctive nucleoli and variable numbers of mitotic figures. Foci of squamoid epithelium are sometimes noted within the epithelial lining. Regressing pilomatricomas display haphazardly arranged foci of basaloid cells and shadow cells as well as an inflammatory infiltrate with multinucleated histiocytic giant cells. Granulation tissue is sometimes noted. Old pilomatricomas reveal no basaloid component but show irregularly shaped, partially confluent masses of shadow cells with foci of calcification or ossification. Melanin deposition, trans-epidermal elimination, and extramedullary hematopoiesis have been described in some pilomatricomas. A peculiar variant with relatively large areas of basaloid cells and small foci of shadow cells (“proliferating pilomatricoma”) is occasionally observed in older adults.
Treatment.
Surgical excision is the most common treatment. Some lesions show spontaneous regression. Local recurrences may occasionally develop after surgical excision. Malignant transformation has been rarely described